Session Information
Date: Sunday, November 12, 2023
Title: (0609–0672) Systemic Sclerosis & Related Disorders – Clinical Poster I: Research
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Although 50% of patients with systemic sclerosis (SSc) present with interstitial lung disease (ILD) at baseline, new onset of ILD can also occur later in the disease. We aimed to compare the phenotypes and prognostic outcome between incident and prevalent ILD in SSc.
Methods: SSc patients from the EUSTAR database were eligible if classified according to the 2013 ACR/EULAR criteria, with available information for ILD on high-resolution computed tomography (HRCT) at baseline and follow-up visits. Patients with pulmonary arterial hypertension on right heart catheterization were excluded.
Based on HRCTs, our population was divided in 3 groups: patients with ILD at baseline (ILD prevalent), patients with new onset of ILD during the follow-up (ILD incident) and patients who remained ILD negative (ILD negative). Disease features were compared between these groups.
ILD groups were tested as a predictor of mortality using multivariable Cox regression with backward selection.
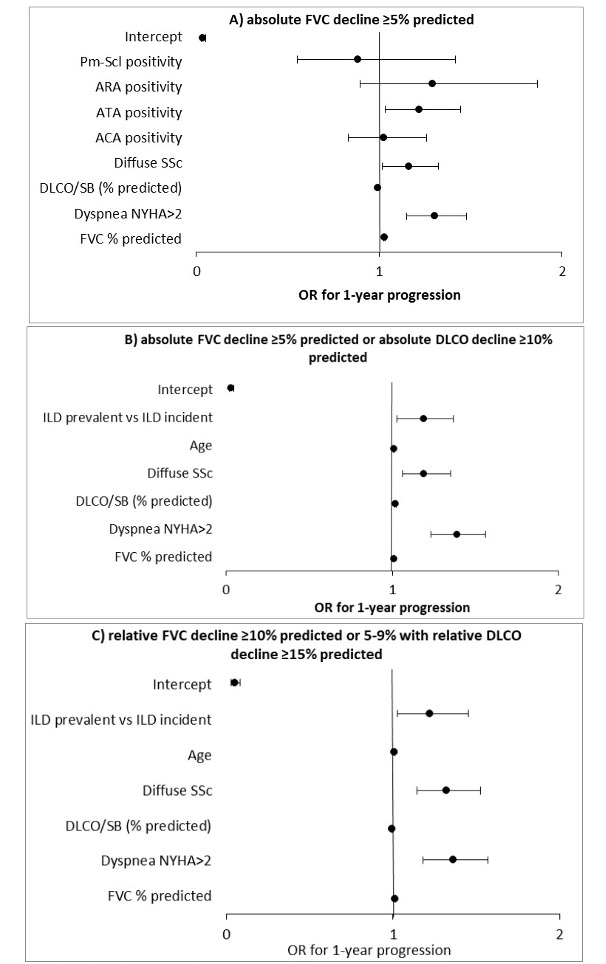
Functional progression of ILD at 12±3 months intervals represented the secondary endpoint. Three different definitions of progression were applied: (A) absolute FVC decline ≥5% predicted, (B) absolute FVC decline ≥5% predicted or absolute DLCO decline ≥10% predicted and (C) relative FVC decline ≥10% predicted or 5-9% with relative DLCO decline ≥15% predicted. Logistic regression with backward selection was used to identify independent predictors, comparing prevalent vs incident ILD.
Known predictors of SSc-ILD progression and mortality were chosen as covariates from the literature and based on expert opinion.
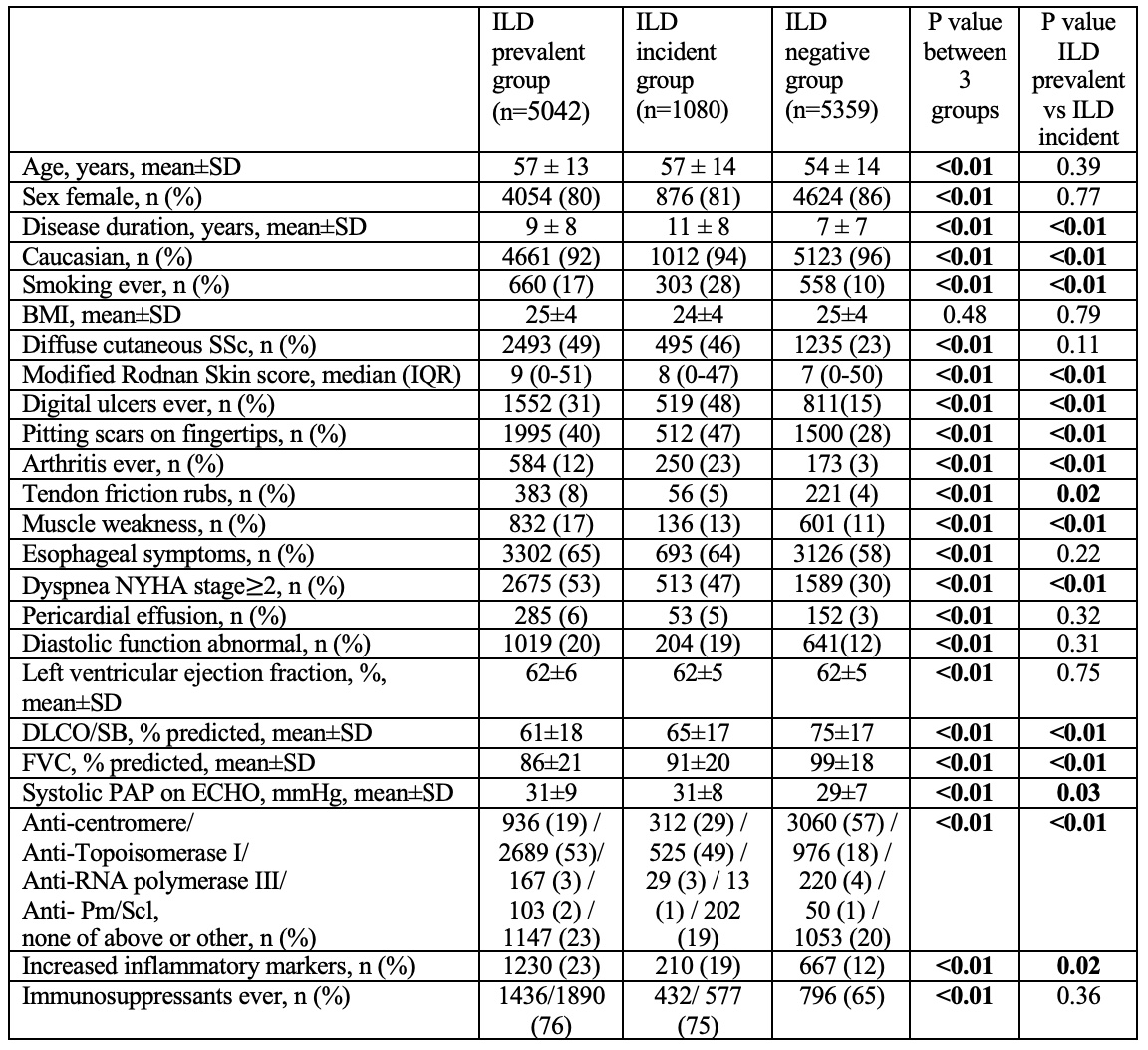
Results: We analyzed 11481 SSc patients, including 5042 (44%) ILD prevalent, 1080 (9%) ILD incident and 5359 (47%) ILD negative patients. In comparison to the prevalent group, the ILD incident group was characterized by a milder functional impairment, higher prevalence of peripheral vascular manifestations, arthritis and smoking ever (Table 1).
During median 3.8 (IQR 1.8-7.3) years follow-up, 753/10157 deaths were recorded, more frequent in the ILD prevalent (67%) compared to ILD incident (22%) or ILD negative (11%)groups (p < 0.01 by Log-rank test).
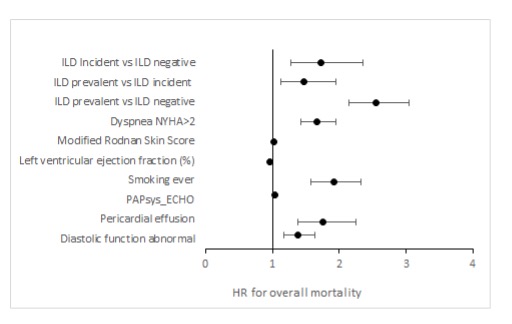
In the Cox regression model adjusted for covariates (Fig.1), the ILD prevalent group showed higher risk of mortality in comparison to both ILD incident (HR 1.47, 95% CI 1.12-1.95) and ILD negative (HR 2.55, 95% CI 2.14-3.05) groups. Notably, the ILD incident had higher risk of mortality than the ILD negative group (HR 1.73, 95% CI 1.27-2.35).
ILD progression was variably observed among 7337 follow-ups of 2803 SSc-ILD patients (in 25% vs 35% vs 19% observations, according to the respective abovementioned definitions).
In comparison to the ILD incident group, the ILD prevalent group showed a higher risk of ILD progression evaluated by definition B (OR 1.18, 95% CI 1.03-1.37) and C (OR 1.21, 95% CI 1.02-1.45) after adjustment for covariates, but it was not confirmed for definition A (Fig.2).
Conclusion: Incident ILD carries a higher risk of mortality compared to ILD negative cases, despite representing a milder phenotype compared to prevalent ILD. Therefore, screening for SSc-ILD should be continued during the follow-up after a negative baseline.
To cite this abstract in AMA style:
Petelytska l, Velauthapillai A, Tofani L, Carreira P, Cuomo G, Hachulla E, Castellvi I, Becvar R, Balbir-Gurman A, Airò P, Litinsky I, Saketkoo L, Vonk M, de Vries-Bouwstra J, Hoffmann-Vold A, Matucci Cerinic m, Distler O, Bruni C. Incident versus Prevalent Interstitial Lung Disease in Systemic Sclerosis in the EUSTAR Database: Different Disease Phenotypes and Prognosis [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/incident-versus-prevalent-interstitial-lung-disease-in-systemic-sclerosis-in-the-eustar-database-different-disease-phenotypes-and-prognosis/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/incident-versus-prevalent-interstitial-lung-disease-in-systemic-sclerosis-in-the-eustar-database-different-disease-phenotypes-and-prognosis/