Session Information
Session Type: Poster Session B
Session Time: 9:00AM-10:30AM
Background/Purpose: Limited information exists on how rates of diagnosis of rheumatic diseases have changed during the COVID-19 pandemic. We compared rates of JIA diagnosis before and during the first year of the US pandemic among commercially insured children.
Methods: Using national commercial health plan data (2016-2021), we identified children under 18 years old with ≥12 months of baseline continuous enrollment without JIA diagnosis or treatment. Incident JIA diagnoses were identified using a combination of ICD-10-CM diagnosis codes (L40.5, M05, M06, M08, or M45) and location and timing of medical services, namely, ≥1 inpatient hospitalization, ≥2 outpatient visits ≥8 weeks apart, or ≥1 outpatient visit PLUS dispensing of JIA medications (NSAID, intra-articular glucocorticoid, oral glucocorticoid or DMARD) within 1 month. Quarters were 90 days in length and anchored on March 1, 2020 (start 2020 Q1). Crude rates (95% confidence intervals (CIs)) of JIA diagnosis per 100,000 enrolled children per quarter 2018-2021 were estimated. Differences based on US region, sex, and age group were explored based on stratified analyses. The incidence rate ratio (95%CI) for JIA diagnosis in the pandemic (Mar 2020-Feb 2021) versus pre-pandemic periods (Mar 2017-Feb 2020) was estimated using Poisson regression, adjusted for age, sex, region, quarter, and census tract-based socioeconomic status using offsets of the log of enrollees per quarter.
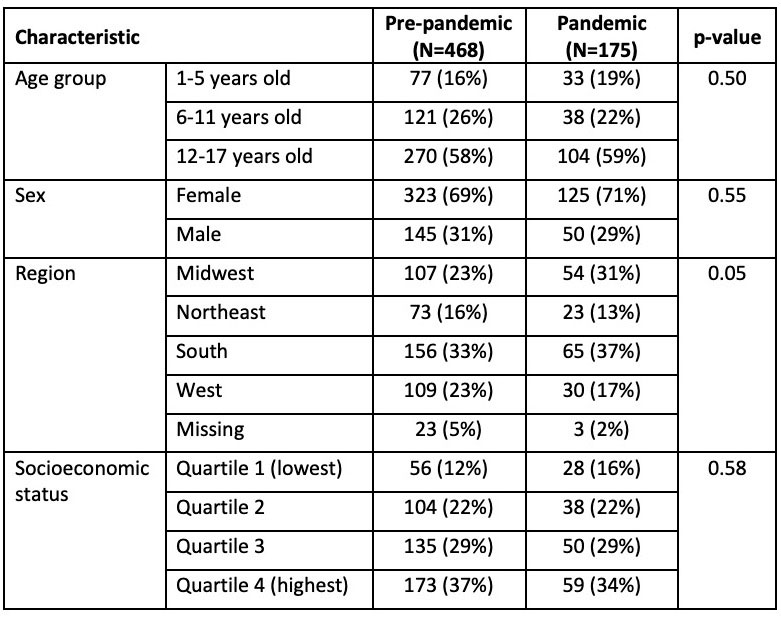
Results: A total of 643 children were diagnosed with JIA during the study period (Table). Crude incident diagnosis rates of JIA dropped from 2.8 per 100,000 children per quarter (95% CI 2.6, 3.0) before the pandemic to 2.0 (95% CI 1.5, 2.4) during the pandemic. Diagnosis rates during the pandemic were lower in Q1 and Q2 and rose in Q3 (coinciding with a national US nadir in COVID-19-associated hospitalizations) before falling again in Q4 (during a subsequent COVID-19 wave in the US) (Figure 1). Declines in JIA diagnosis were more apparent in the US Northeast and West and among older children (Figure 2). After adjustment for covariates, JIA diagnoses fell by 30% during the pandemic compared to the prior 3 years (IRR 0.70, 95% CI 0.59-0.83).
Conclusion: Compared with the pre-pandemic period, JIA was diagnosed 30% less often during the first year of the pandemic among commercially insured children in the US. The rebound in diagnosis rates in the fall of 2020 and the heterogeneity across US regions suggest that these declines were due at least partly to pandemic-related changes in healthcare utilization and access to care. More research is needed to understand the underlying reasons for the observed changes in JIA diagnosis, whether all types of JIA were affected similarly, and whether pandemic-related delays in diagnosis led to worse outcomes at a population level.
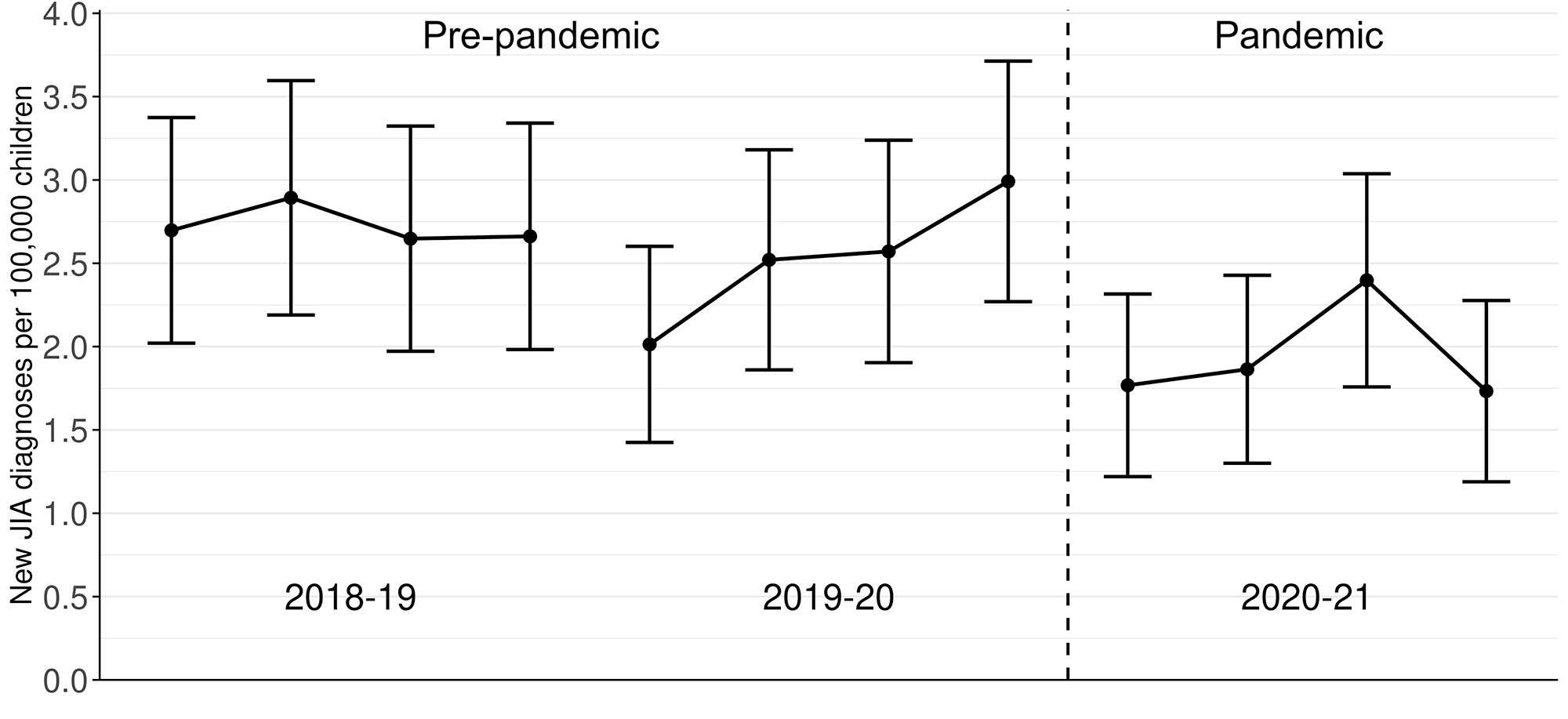
Crude rates (markers) with 95% confidence intervals (bars) were estimated for new JIA diagnoses per 100,000 enrolled children per quarter, Mar 2018-Feb 2021. The pre-pandemic and pandemic periods are shown separated by a vertical dashed line.
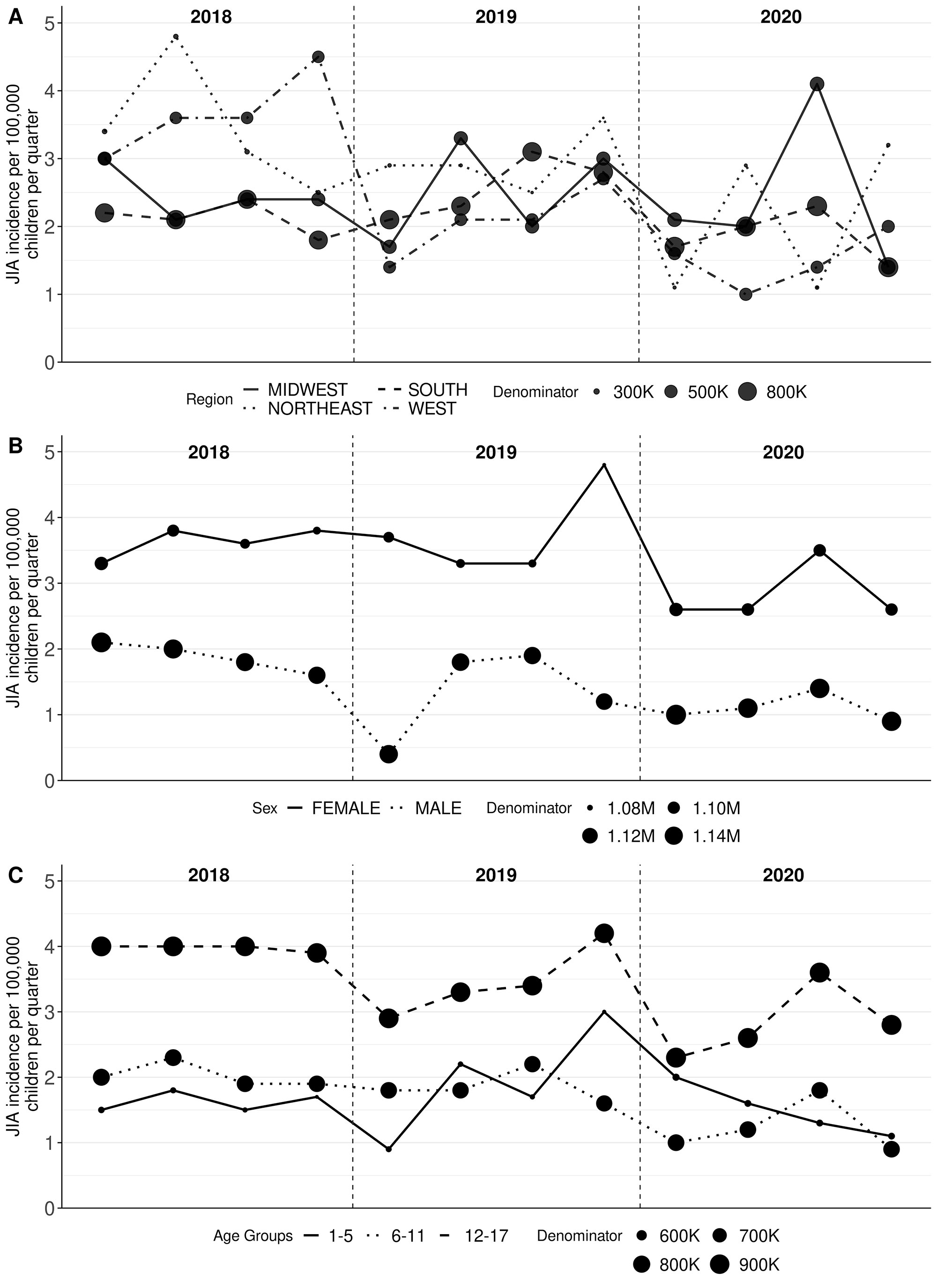
Crude rates were estimated for new JIA diagnoses per 100,000 enrolled children per quarter, Mar 2018-Feb 2021, stratified by region (A), sex (B), and age group (C). Marker sizes are proportional to the sizes of the respective subpopulations.
To cite this abstract in AMA style:
Horton D, Neikirk A, Yang Y, Huang C, Crystal S, davidow a, Haynes K, Gerhard T, Rose C, Strom B, Parlett L. Incidence of Juvenile Idiopathic Arthritis During the COVID-19 Pandemic: An Analysis of National United States Administrative Claims Data [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/incidence-of-juvenile-idiopathic-arthritis-during-the-covid-19-pandemic-an-analysis-of-national-united-states-administrative-claims-data/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/incidence-of-juvenile-idiopathic-arthritis-during-the-covid-19-pandemic-an-analysis-of-national-united-states-administrative-claims-data/