Session Information
Session Type: Poster Session C
Session Time: 1:00PM-3:00PM
Background/Purpose: We presented preliminary data in 2021 to support the feasibility of using a semi-quantitative chest CT scoring system (Pediatric Rheumatologic Diffuse Lung Disease Score [PRDLDS]) to evaluate the prevalence of diffuse lung disease (DLD) assessed by CT in pediatric rheumatologic patients. Our initial scoring data, after preliminary radiologic training, demonstrated mild parenchymal disease and no emphysema, but high inter-rater variability for parenchymal scoring in such patients. In addition, we noted inaccurate scoring based on the pulmonary hypertension (PHT) domain of the PRDLDS. The purpose of this follow-up study was to determine the effectiveness to improve the diagnostic performance of pediatric radiology scorers in evaluating lung disease in PR patients by providing more extensive training with a modified PRDLDS scoring system without pulmonary hypertension and emphysema (MPRDLDS, Table 1).
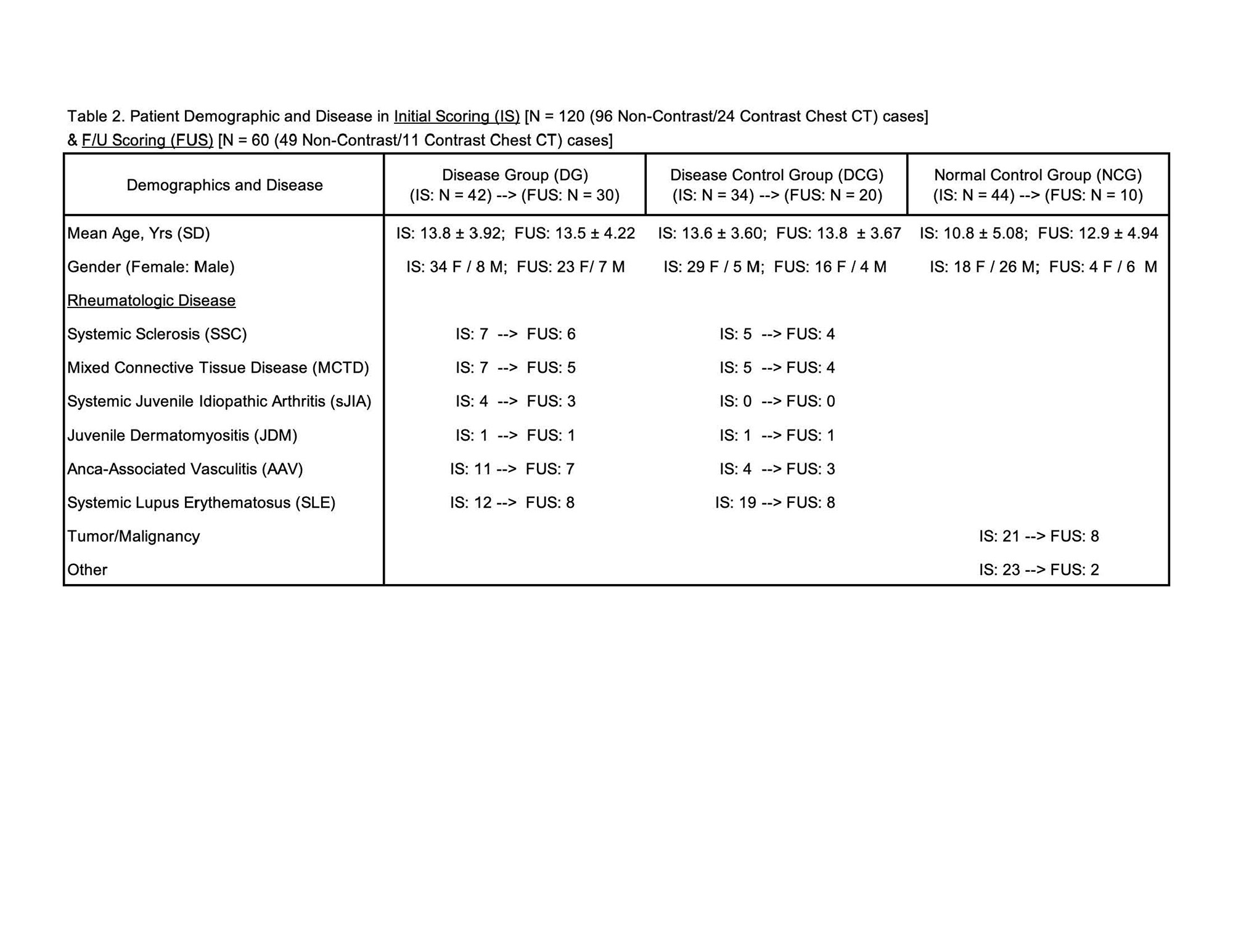
Methods: Initially three radiologists with varying DLD scoring experience independently read 1-2 mm inspiratory chest CT scans (96 non-contrast/24 Contrast) in 120 pediatric subjects (DG: N=42 PR patients with DLD; DCG: N=34 PR patients without DLD; and NCG: N=44 pediatric normal control subjects with chest CT scans) from 3 medical centers (Children’s Hospital of LA, Stanford Children’s Health, Mayo Clinic). After more extensive training with these radiologists using the MPRDLDS, they read 60 cases of the original 120 cases (DG: N=30; DCG: N=20; and NCG: N=10). We compared the scores before (N=120 cases) and after (N=60 cases) this training. Demographic and disease representation of the cases was similar between the groups (Table 2).
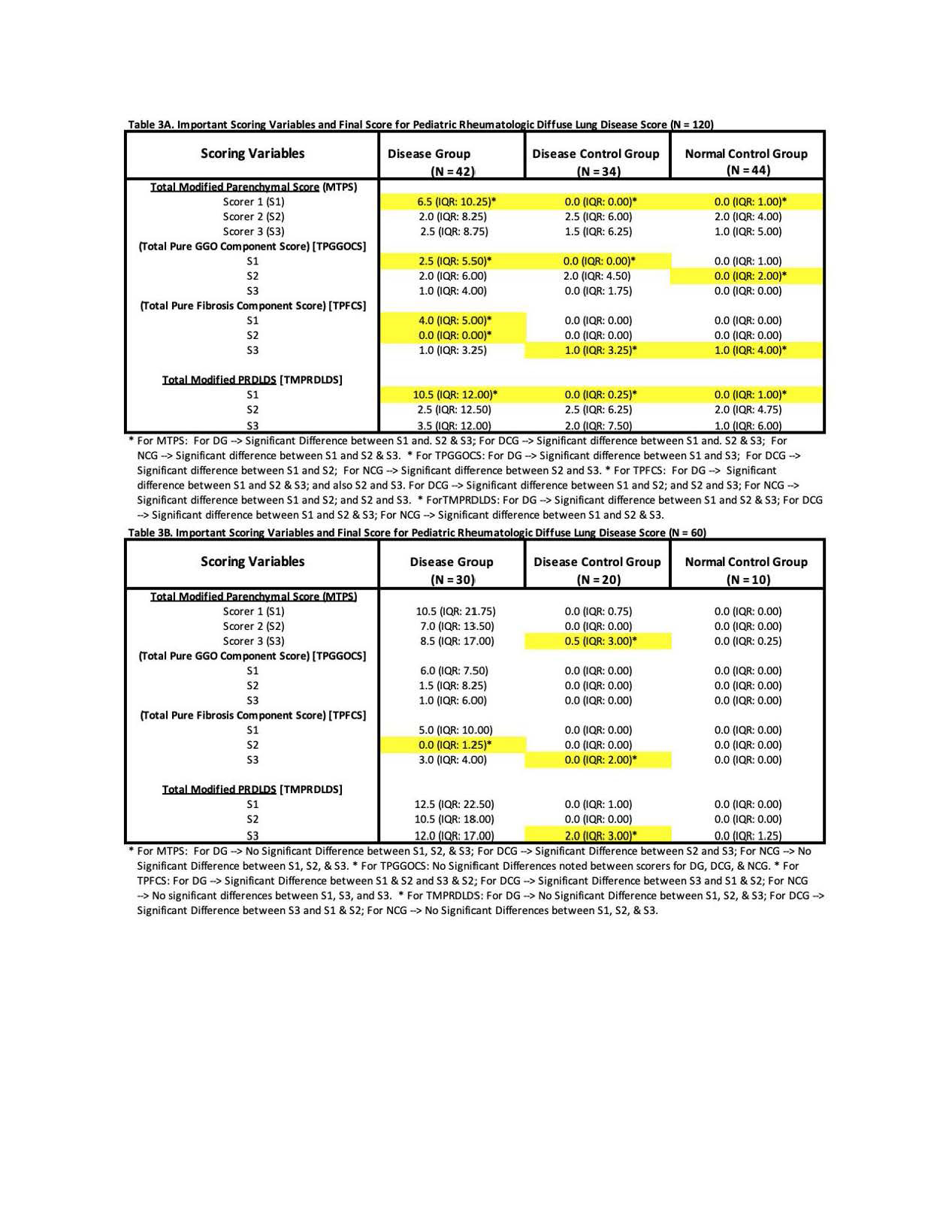
Results: With further training, there was overall more pronounced disease detected by all readers for the DG noted from initial scoring (N=120) to the follow-up scoring (N=60); there was also no significant difference between readers for aggregate parenchymal scores (MTPS) and total MPRDLDS (Table 3). In addition, control groups (DCG, DCG) previously evaluated to have minimal to no DLD were now evaluated to have essentially no DLD.
Conclusion: Semi-quantitative scoring using the MPRDLDS with more extensive training is a feasible tool to detect the extent of DLD in PR patients. Our data revealed that our PR patients have mild DLD which is primarily contributed by parenchymal disease. Due to the mild nature of this pulmonary disease, more extensive training of the readers with the MPRDLDS scoring system is crucial.

To cite this abstract in AMA style:
Cidon M, Newman B, Robinson T, Iskander P, Thacker P, Zucker E, Lee T, Moats R. Improving Radiologic Interpretation of Diffuse Lung Disease in Pediatric Rheumatologic (PR) Patients Using Trained Scoring with Semi-quantitative Chest Computed Tomography (CT) Analysis [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/improving-radiologic-interpretation-of-diffuse-lung-disease-in-pediatric-rheumatologic-pr-patients-using-trained-scoring-with-semi-quantitative-chest-computed-tomography-ct-analysis/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/improving-radiologic-interpretation-of-diffuse-lung-disease-in-pediatric-rheumatologic-pr-patients-using-trained-scoring-with-semi-quantitative-chest-computed-tomography-ct-analysis/