Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
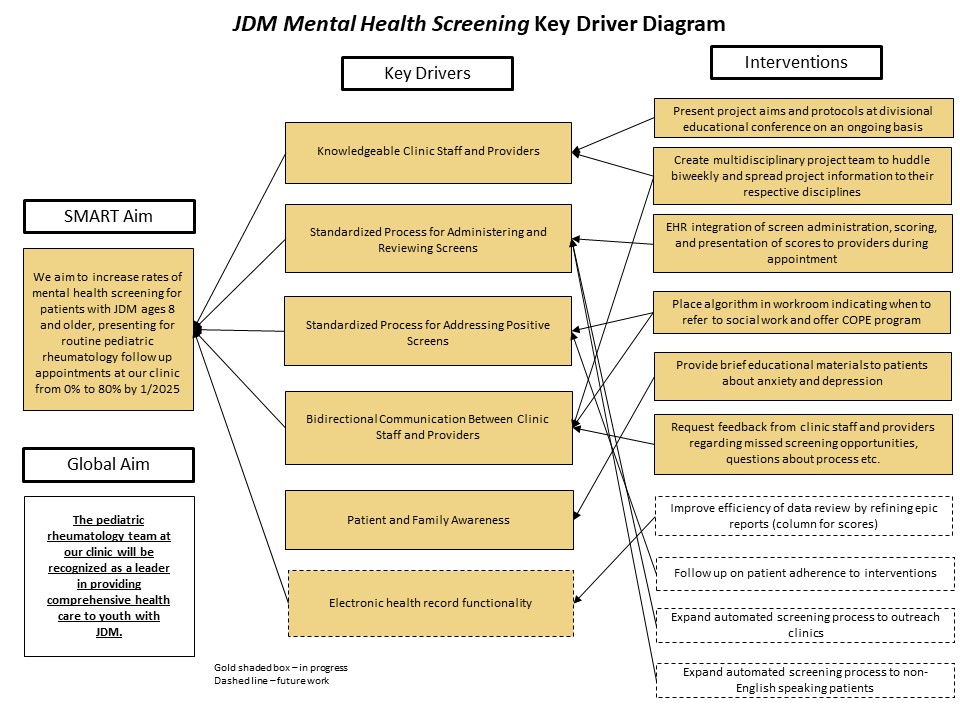
Background/Purpose: The negative impact of juvenile dermatomyositis (JDM) on emotional health is well-recognized. Barriers to appropriate mental health treatment include limited availability of providers and challenges with coordination of care. The purpose of our quality improvement project is to improve mental health care for youth with JDM by first implementing routine screening for anxiety and depression, followed by integration of initial mental health treatment into our pediatric rheumatology clinic. The aim of this phase was to increase mental health screening for patients with JDM aged 8 years and older, presenting for routine pediatric rheumatology follow up appointments from 0% to 80% by January 2025.
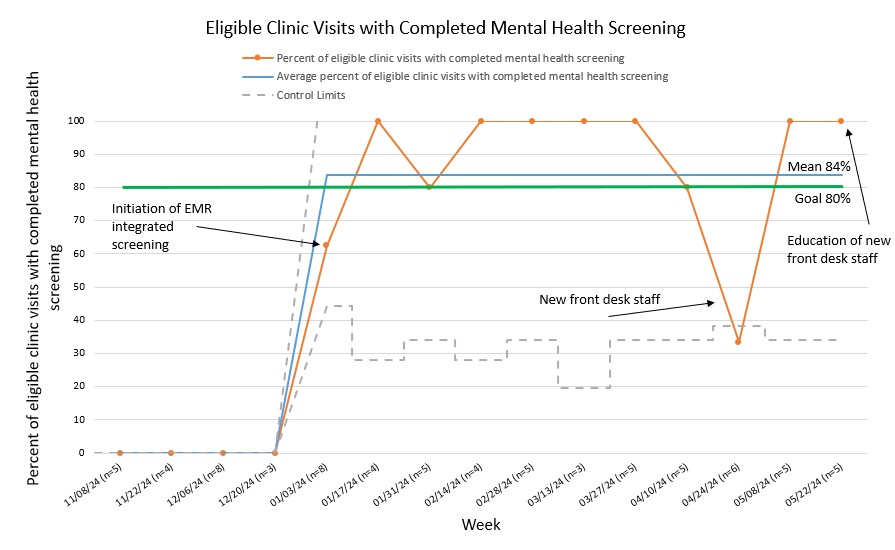
Methods: Patients with JDM seen for routine follow-up in our pediatric rheumatology clinic from January 3, 2024 through June 4, 2024 were given validated mental health screening tools. The Screen for Childhood Anxiety and Related Emotional Disorders (SCARED) was given to children aged 8 years or older. For children aged 12 years and older, the Patient Health Questionnare-9 modified for adolescents (PHQ-A) was also given. Screens were administered on a tablet given to patients at check in by front desk staff. The electronic health record (EHR) automatically identified patients, assigned and scored screens, and clearly displayed screen results to providers at the time of visit. Our team previously implemented a similar process for standardized depression screening for youth with systemic lupus erythematosus. A key driver diagram was used to plan potential interventions (Figure 1). Plan-Do-Study-Act (PDSA) cycles were used to prepare, implement, and evaluate interventions. Interventions targeted the key drivers of knowledgeable clinic staff and providers, standardized processes for administering, reviewing, and addressing screens, and patient and family awareness. Statistical process control methods were used for data analysis. Our primary outcome measure was the percent of eligible patient encounters where age-appropriate mental health screening was completed.
Results: The percentage of eligible patient encounters where age-appropriate mental health screening was completed increased from 0% to 84% after implementation of our automated screening process (Figure 2). This represents special cause variation as evidenced by a data shift on our statistical process control chart. We had one data point outside our control limits representing special cause variation in the direction opposite our goal. This occurred when patients were not given tablets at appointment check in by newly hired front desk staff. We then provided education for new front desk staff and made plans to improve the new hire onboarding process.
Conclusion: A high rate of standardized mental health screening for youth with JDM was achieved and maintained via an automated EHR integrated system. Establishing a highly reliable screening system is a critical first step in improving mental health care for this vulnerable population of youth. Next steps include integration of initial mental health interventions in the pediatric rheumatology clinic.
To cite this abstract in AMA style:
Datyner E, Buckley L, Nelson B, Davis A. Improving Mental Health Care for Youth with Juvenile Dermatomyositis Through Integration of Mental Health Screening into Pediatric Rheumatology Clinic [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/improving-mental-health-care-for-youth-with-juvenile-dermatomyositis-through-integration-of-mental-health-screening-into-pediatric-rheumatology-clinic/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/improving-mental-health-care-for-youth-with-juvenile-dermatomyositis-through-integration-of-mental-health-screening-into-pediatric-rheumatology-clinic/