Session Information
Session Type: Poster Session A
Session Time: 8:30AM-10:30AM
Background/Purpose: Coronary microvascular dysfunction (CMVD) has been described in patients with autoimmune rheumatic disease (ARD). By noninvasive evaluation of myocardial blood flow (MBF) and myocardial flow reserve (MFR) quantification, positron emission tomography (PET) imaging has emerged as the noninvasive gold standard CMVD assessment. However, to date, no large studies have evaluated PET-derived MFR in ARD patients. It is also unknown whether MFR can predict adverse events in this population.
Methods: Patients with ARD without coronary artery disease who underwent dynamic rest-stress 82Rubidium PET from 05/2012-05/2019 for a clinical indication were retrospectively studied and compared to patients without ARD matched for age, gender and comorbidities. The association between MFR and a composite endpoint of mortality or myocardial infarction (MI) or heart failure (HF) admission was evaluated with time to event and Cox-regression analyses.
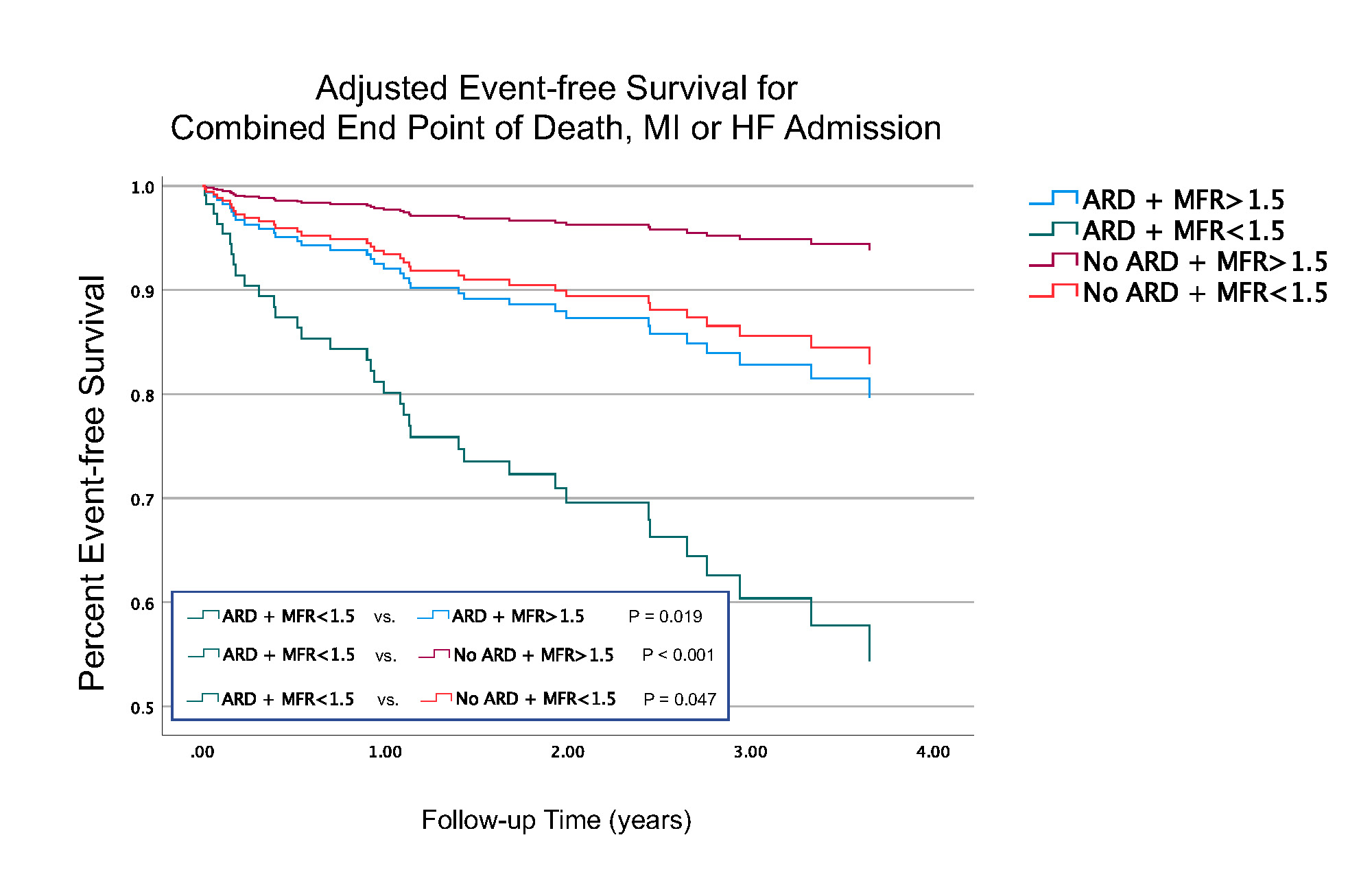
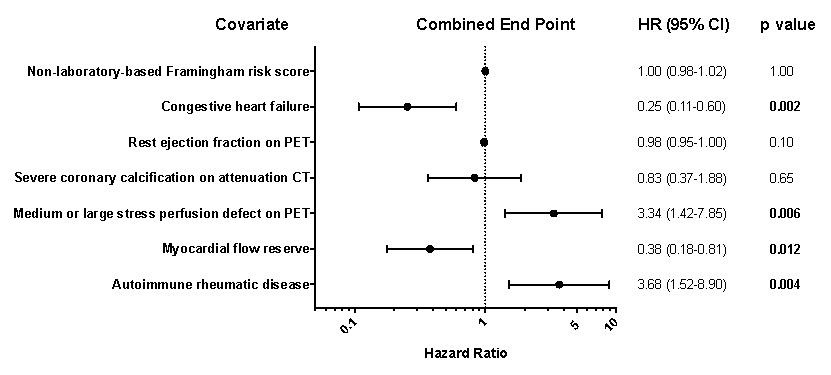
Results: In 101 patients with ARD (88% female, age: 62±10 years), stress MBF did not significantly differ between patients with ARD (median with interquartile range [IQR], 1.68 [IQR: 1.39 – 2.07]) compared to those without ARD (1.49 [IQR: 1.26 – 1.93]) (Figure 1A). Conversely, rest MBF was significantly higher in ARD patients (1.00 [IQR: 0.84 – 1.21]) compared to those without an ARD diagnosis (0.80 [IQR: 0.68 – 0.99]) (Figure 1B). Consequently, MFR was significantly reduced in ARD patients compared to patients without ARD (1.68 [IQR: 1.34 – 2.05] vs. 1.86 [IQR: 1.58 – 2.28]) (Figure 1C). MFR did not differ among subtypes of ARDs. During the median follow-up of 3.8 years, there were twelve deaths, two MIs and 18 HF admissions in ARD patients. In survival analysis, patients with ARD and low MFR (MFR< 1.5) had decreased event-free survival for the combined endpoint, when compared to patients with and without ARD and normal MFR (MFR >1.5) and when compared to patients without ARD and low MFR, after adjustment for the non-laboratory-based Framingham risk score, rest left ventricular ejection fraction, severe coronary calcification, and the presence of medium/large perfusion defects (Figure 2). In Cox-regression analysis, ARD diagnosis and MFR were both independent predictors of adverse events in ARD patients along with congestive HF diagnosis and presence of medium/large stress perfusion defects on PET (Figure 3).
Conclusion: Patients with ARD have significantly reduced PET MFR compared to age-, gender- and comorbidity-matched patients without ARD. Reduced PET MFR and ARD diagnosis are both independent predictors of adverse outcomes.

To cite this abstract in AMA style:
Feher A, Boutagy N, Oikonomou E, Liu Y, Miller E, Sinusas A, Hinchcliff M. Impaired Myocardial Flow Reserve on 82Rubidium Positron Emission Tomography Imaging Predicts Adverse Events in Patients with Autoimmune Rheumatic Disease [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/impaired-myocardial-flow-reserve-on-82rubidium-positron-emission-tomography-imaging-predicts-adverse-events-in-patients-with-autoimmune-rheumatic-disease/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/impaired-myocardial-flow-reserve-on-82rubidium-positron-emission-tomography-imaging-predicts-adverse-events-in-patients-with-autoimmune-rheumatic-disease/