Session Information
Session Type: Poster Session A
Session Time: 8:30AM-10:30AM
Background/Purpose: To investigate the association between Raynaud phenomenon (RP) and coronary microvascular dysfunction, we measured myocardial flow reserve (MFR) using positron emission tomography/computed tomography (PET/CT) in patients with primary and secondary RP and controls.
Methods: Patients with RP and matched controls who underwent dynamic rest-stress 82-Rubidium PET/CT from 09/2012-09/2019 for evaluation of chest pain or dyspnea were studied. Differences in heart rate-blood pressure product corrected MFR and clinical predictors of reduced MFR (< 2.0) were determined (Figure 1.).
Results: 49 patients (80% female, 65 ± 11 years) with RP (11 with primary RP, 18 with systemic sclerosis (SSc) and 20 with other autoimmune diagnoses (AID, n=6 systemic lupus erythematosus, n=6 rheumatoid arthritis, n=4 overlap syndrome, n=2 Sjogren’s syndrome, n=2 inflammatory arthritis), 49 patients without RP matched for age, gender and cardiovascular co-morbidities (78% female, 64 ± 13 years) and 14 healthy controls (50% female, 35 ± 5 years) were studied. Primary RP patients, healthy participants and matched control patients had comparable MFR (Figure 2.). In secondary RP patients, only those with underlying SSc had significantly reduced MFR (1.62 ± 0.32) compared to healthy participants (p=0.01, 2.22 ± 0.44) and to matched controls (p=0.03, 2.06 ± 0.61). In univariate (Fig 3A) and multivariable logistic regression (Figure 3B), only SSc was a significant predictor of reduced MFR. We have also identified a correlation between time since autoimmune disease diagnosis and MFR (r= -0.37; 95% CI: -0.61 to -0.09; p=0.01).
Conclusion: Our findings suggest that only secondary, not primary, RP is associated with reduced MFR, and that SSc-RP patients have reduced MFR compared to primary RP and other autoimmune disease patients. Larger prospective studies are warranted to fully elucidate the prognostic value of MFR in patients with secondary RP.
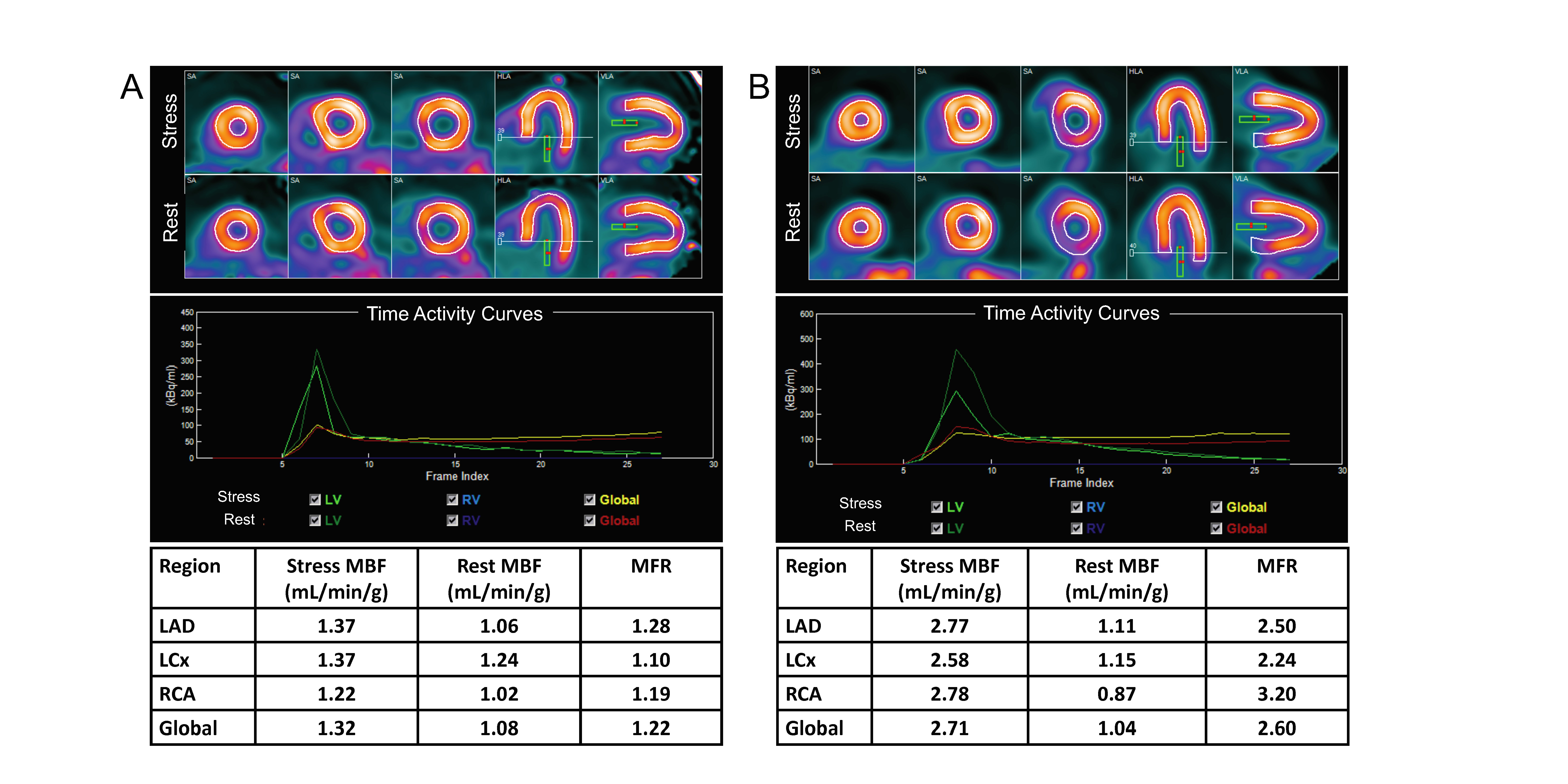 Fig1.jpeg”
Fig1.jpeg”
 Fig3.jpeg”
Fig3.jpeg”
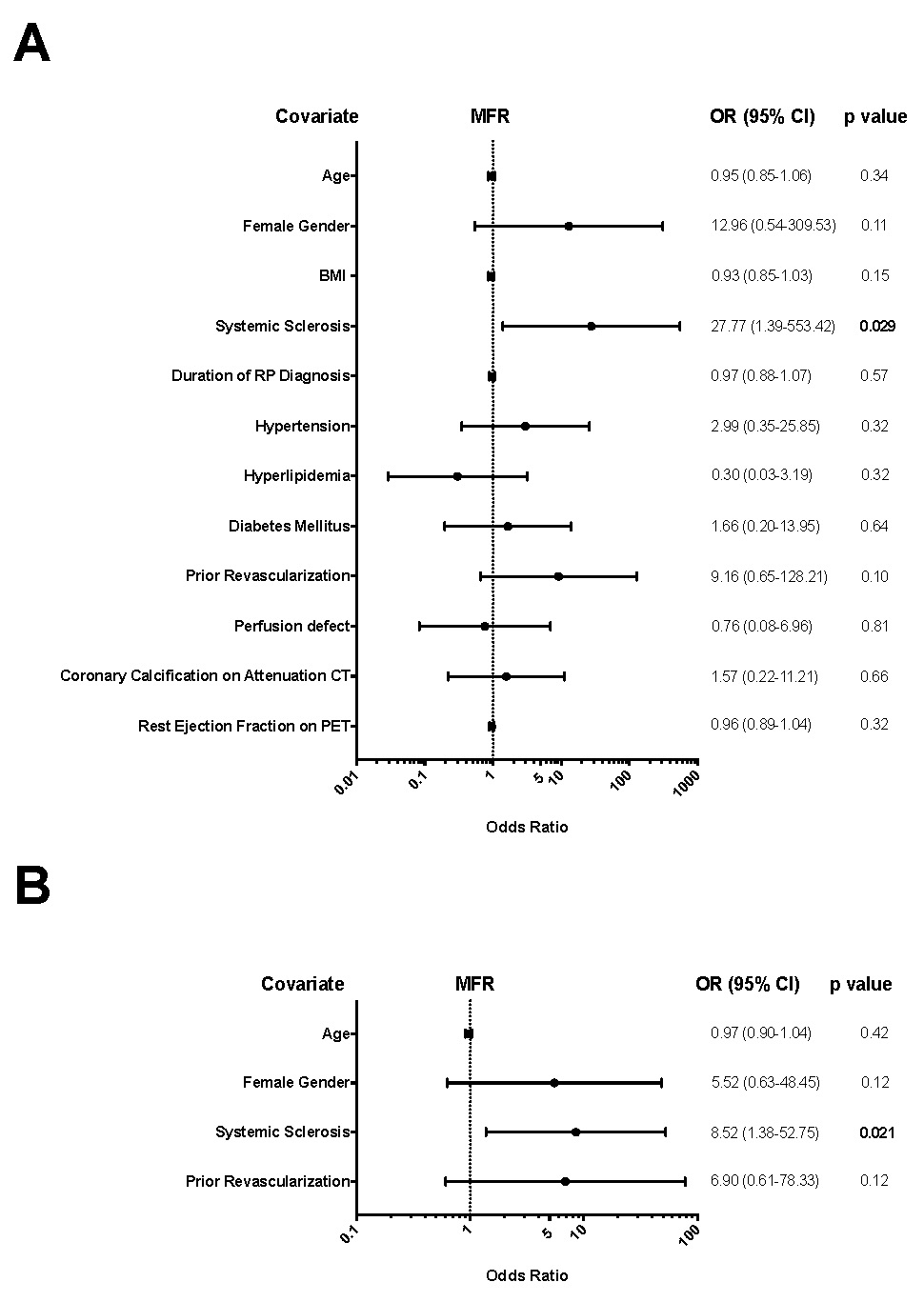 Fig4.jpeg”
Fig4.jpeg”
To cite this abstract in AMA style:
Feher A, Boutagy N, Oikonomou E, Thorn S, Liu Y, Miller E, Sinusas A, Hinchcliff M. Impaired Myocardial Flow Reserve on 82Rubidium Positron Emission Computed Tomography in Patients with Systemic Sclerosis [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/impaired-myocardial-flow-reserve-on-82rubidium-positron-emission-computed-tomography-in-patients-with-systemic-sclerosis/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/impaired-myocardial-flow-reserve-on-82rubidium-positron-emission-computed-tomography-in-patients-with-systemic-sclerosis/