Session Information
Date: Tuesday, October 28, 2025
Title: (2470–2503) Systemic Sclerosis & Related Disorders – Clinical Poster III
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Cardiovascular death ranks as the second leading cause of mortality related to systemic sclerosis (SSc), with coronary microvascular dysfunction (CMVD) likely contributing to this outcome. Positron emission tomography (PET) myocardial perfusion imaging (MPI) has emerged as the noninvasive gold standard for assessing myocardial blood flow (MBF) and myocardial flow reserve (MFR), offering unparalleled accuracy in detecting CMVD. We undertook the present study to explore the relationship between vasodilators, SSc disease-modifying antirheumatic drugs and CMVD in SSc patients.
Methods: We conducted a retrospective study involving patients diagnosed with SSc who underwent 82-rubidium PET MPI from July 2016 to April 2025 for clinical indications. These patients were compared to a control group without connective tissue disease, matched 3:1 for age, sex, body mass index (BMI), cardiovascular comorbidities, and presenting symptoms. Differences between groups were analyzed using the Chi-Square test and the Wilcoxon rank-sum test. Univariable and multivariable logistic regression models were used to assess SSc-related predictors of clinically significant reduced MFR (< 2.0). Parameters with p< 0.05 in univariable analysis were included in multivariable model. Statistical analyses were performed with R version 4.4.2.
Results: The final cohort included 67 patients with SSc (87% female, mean age: 61 years, 14 with diffuse cutaneous SSc, disease duration: 12 ± 10 years) and 201 matched controls (Table 1). While stress MBF was not significantly different between SSc patients and controls (2.47 [IQR: 1.99-2.82] vs. 2.43 [IQR: 1.91-3.04] ml/g/min, p=0.85), rest MBF was significantly higher in SSc patients (1.14 [IQR: 0.92-1.37] vs. 1.00 [IQR: 0.78-1.24] ml/g/min, p=0.01) and MFR was significantly lower (2.17 [IQR: 1.84-2.57] vs. 2.44 [IQR: 1.96-2.96], p=0.01, Figure 1). Rates of abnormal perfusion, ischemic ECG changes, stress left ventricular ejection fraction, and visual coronary calcium scores were comparable between SSc patients and controls. In SSc patients, multivariable analysis identified mycophenolate mofetil (MMF) use as associated with significantly reduced odds for abnormal MFR (odds ratio [OR]: 0.09 [95% confidence interval[CI]: 0.01-0.56], p=0.017), whereas calcium channel blocker use (OR: 7.77 [95% CI: 1.93-42.53], p=0.008) and statin use (OR: 7.14 [95% CI: 1.86-36.87], p=0.008) were associated with higher odds of abnormal MFR (Table 2).
Conclusion: Patients with SSc exhibit significantly reduced PET-derived MFR compared to matched controls, indicating higher CMVD prevalence. Our finding of a significant association between calcium channel blocker or statin use and abnormal MFR may reflect more severe systemic microvascular disease. Conversely, the observed association between MMF use and lower incidence of reduced MFR suggests potential benefits through mechanisms such as cytokine suppression, antioxidant activity, or enhanced nitric oxide production. Further studies are warranted to validate these findings and to elucidate the effects of MMF on microvascular function in SSc.
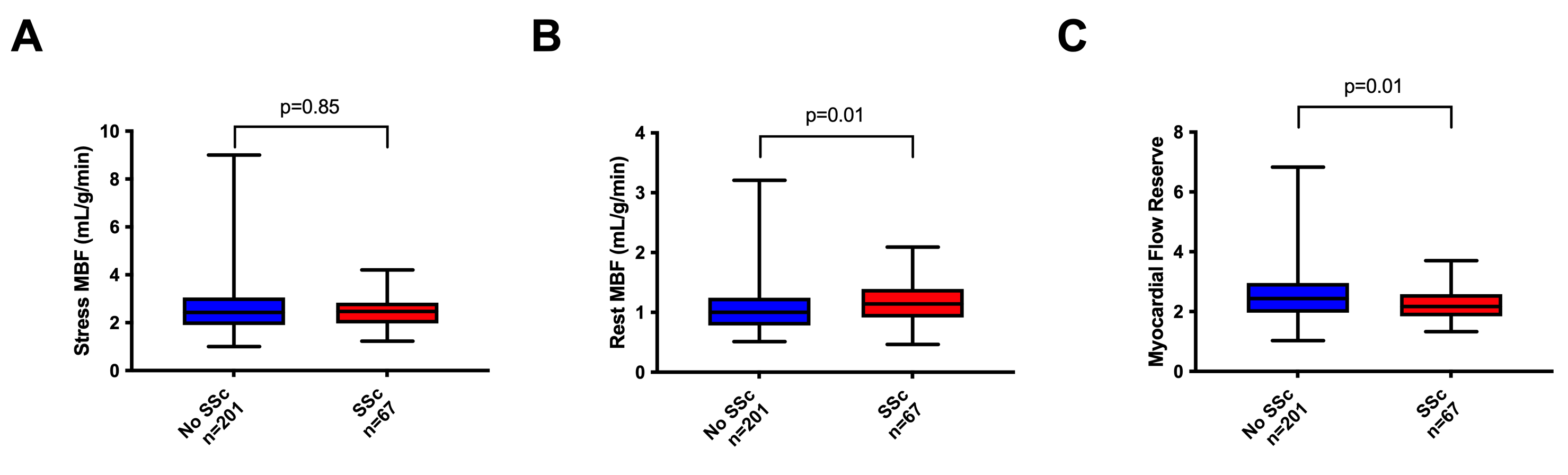 Table 1. Baseline and imaging characteristics in systemic sclerosis (SSC) patients and matched controls.
Table 1. Baseline and imaging characteristics in systemic sclerosis (SSC) patients and matched controls.
.jpg) Figure 1. Stress and rest myocardial blood flow (MBF) and myocardial flow reserve in SSc patients and controls
Figure 1. Stress and rest myocardial blood flow (MBF) and myocardial flow reserve in SSc patients and controls
.jpg) Table 2. Univariable and multivariable logistic regression for prediction of reduced myocardial flow reserve ( < 2.0)
Table 2. Univariable and multivariable logistic regression for prediction of reduced myocardial flow reserve ( < 2.0)
To cite this abstract in AMA style:
Feher A, Emokpae M, Koyi B, Csecs I, Gunes B, Sinusas A, Hinchcliff M. Impaired Myocardial Flow Reserve on 82-Rubidium Positron Emission Tomography in Patients with Systemic Sclerosis [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/impaired-myocardial-flow-reserve-on-82-rubidium-positron-emission-tomography-in-patients-with-systemic-sclerosis/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/impaired-myocardial-flow-reserve-on-82-rubidium-positron-emission-tomography-in-patients-with-systemic-sclerosis/