Session Information
Date: Sunday, November 12, 2023
Title: (0229–0251) Metabolic & Crystal Arthropathies – Basic & Clinical Science Poster I
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Gout is associated with increased cardiovascular risk (CVR). Traditional CVR factors (CVRF) are frequently present in patients with gout, further worsening the prognosis. Several studies have shown that clinical nurse specialist (CNS) contributes effectively to the management of gout. To analyze the detection of CVRF in patients with gout in a rheumatology consultation with CNS and to evaluate short-term changes after a targeted approach.
Methods: Patients with gout according to ACR/EULAR 2015 criteria referred from Primary/Specialized Care due to poor control of the disease. At the first visit, demographic and clinical variables were collected: age, sex, smoking, alcohol, duration of gout, tophi, comorbidities, urate-lowering treatment (ULT) and concomitant drugs. A blood test and review of previous were performed, as well as measurement of blood pressure (BP), weight and abdominal circumference. Nurse-managed calls were made to monitor home measurements and check adherence/tolerance to pharmacological (start/adjustment of ULT, antihypertensive, lipid-lowering and antidiabetic drugs) and non-pharmacological approach (gout education, dietary/lifestyle recommendations) initiated, according to EULAR recommendations for CVR management in rheumatic diseases. We count on multidisciplinary collaboration with other specialists. After 6 months, an in-person visit was made with the same measurements to determine potential changes. A descriptive analysis of the sample was performed. Wilcoxon test was used to evaluate the variation in the parameters studied. The outcome variable was determined as improvement vs no improvement of the dependent variable. χ2 and Mann Whitney U tests were used to evaluate the differences.
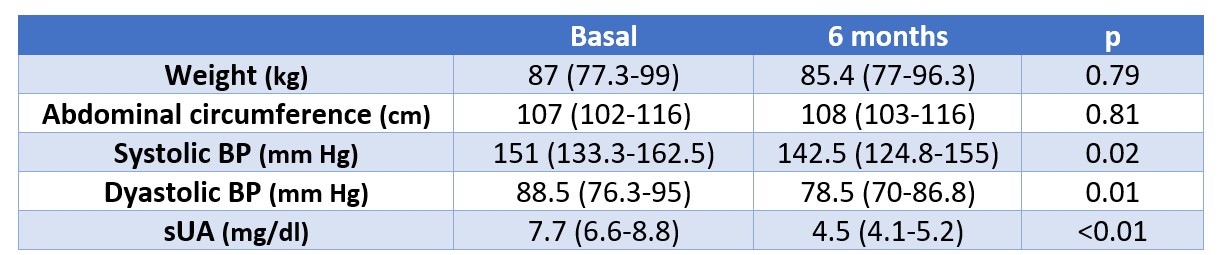
Results: Forty patients who met the inclusion criteria were included. Ninety-eight percent were male, with a median age of 66 (58-75) years, severe gout (83% tophaceous, median duration 7 years) and marked presence of CVRF (hypertension 78%, dyslipidemia 55%, smoking 23%, diabetes 23%), some of them previously undetected (10% hypertensive, 3% dyslipidemic, 3% diabetic), and related comorbidities (ischemic heart disease 8%, cerebrovascular disease 5%, chronic kidney disease 20%). Fifty-five percent were not taking ULT and 53% used NSAIDs on a regular basis. At the first visit, ULT was started/adjusted in 95% of patients, antihypertensive in 15%, lipid-lowering drugs in 13%, and anti-diabetes drugs in 8%. At 6 months, there was a significant improvement in sUA and BP, and a non-statistically significant weight reduction (Table). Serum uric acid (sUA) target was achieved in 93% of patients (37/40 < 6 mg/dl, 29/40 < 5 mg/dl). The use of NSAIDs was reduced to 5%. Four out of 9 smokers quit. Systolic BP improved in 73% of patients and diastolic BP in 70%. Dietary and habit modifications, therapeutic adjustments and multidisciplinary care were significantly associated with improved BP (p=0.02).
Conclusion: In patients with difficult-to-treat gout and high CVR, combined intervention with CNS allows substantial short-term changes in CVRF, drastic reduction in NSAID consumption and a high percentage of success in achieving sUA target.
To cite this abstract in AMA style:
Gomez C, Cardoso Peñafiel P, Angel-Sesmero J, Novella-Navarro M, Calvo-Aranda E. Impact of Combined Intervention with Clinical Nurse Specialist in the Management of Cardiovascular Risk in Patients with Gout [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/impact-of-combined-intervention-with-clinical-nurse-specialist-in-the-management-of-cardiovascular-risk-in-patients-with-gout/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/impact-of-combined-intervention-with-clinical-nurse-specialist-in-the-management-of-cardiovascular-risk-in-patients-with-gout/