Session Information
Date: Sunday, November 12, 2023
Title: (0691–0721) Vasculitis – Non-ANCA-Associated & Related Disorders Poster I
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Constrictive pericarditis (CP) is a type of diastolic heart failure characterized by impaired cardiac filling due to the presence of an inelastic pericardium. Histologically, the pericardium exhibits fibrotic and thickened features. While tuberculosis remains the primary cause of CP in developing countries, idiopathic CP predominates in North America and Europe. The extent to which idiopathic CP patients may belong to the spectrum of IgG4-related disease remains unknown. Therefore, our objective was to determine the number of idiopathic CP patients meeting histopathological criteria for IgG4-RD.
Methods: Clinical records of patients with CP attended between 1987-2020 were reviewed. Those without a biopsy or with a known etiology of CP were excluded. Pericardial biopsies were analyzed in search of dense lymphoplasmacytic infiltrate, storiform fibrosis, and obliterative phlebitis. Immunohistochemistry for IgG and IgG4 was performed. The number of IgG+ and IgG4+ plasma cells and the IgG4/IgG ratio were determined according to the International Consensus on Pathology (ICP) of IgG4-RD. According to the ICP, cases were classified as highly suggestive, probable histopathological characteristics, or insufficient histopathological evidence. The Comprehensive Diagnostic Criteria for IgG4-RD (CDCI) and the 2019 ACR/EULAR classification criteria (AECC) were also applied. Clinical characteristics were extracted from the patients’ medical records.
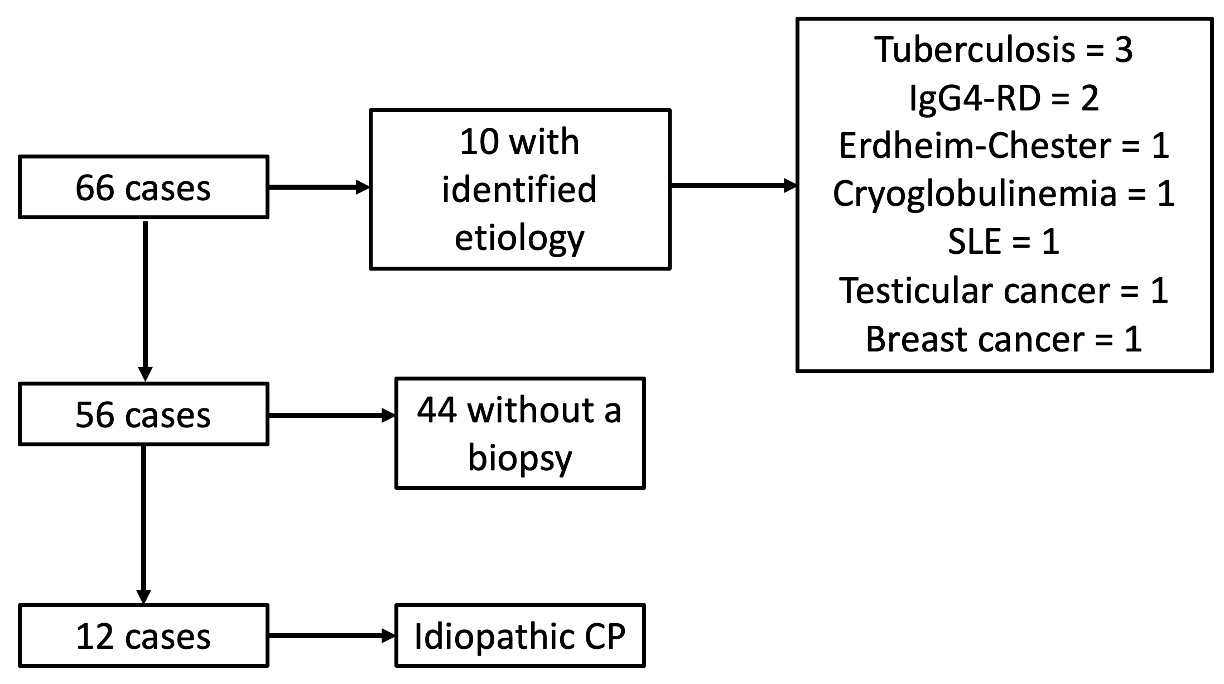
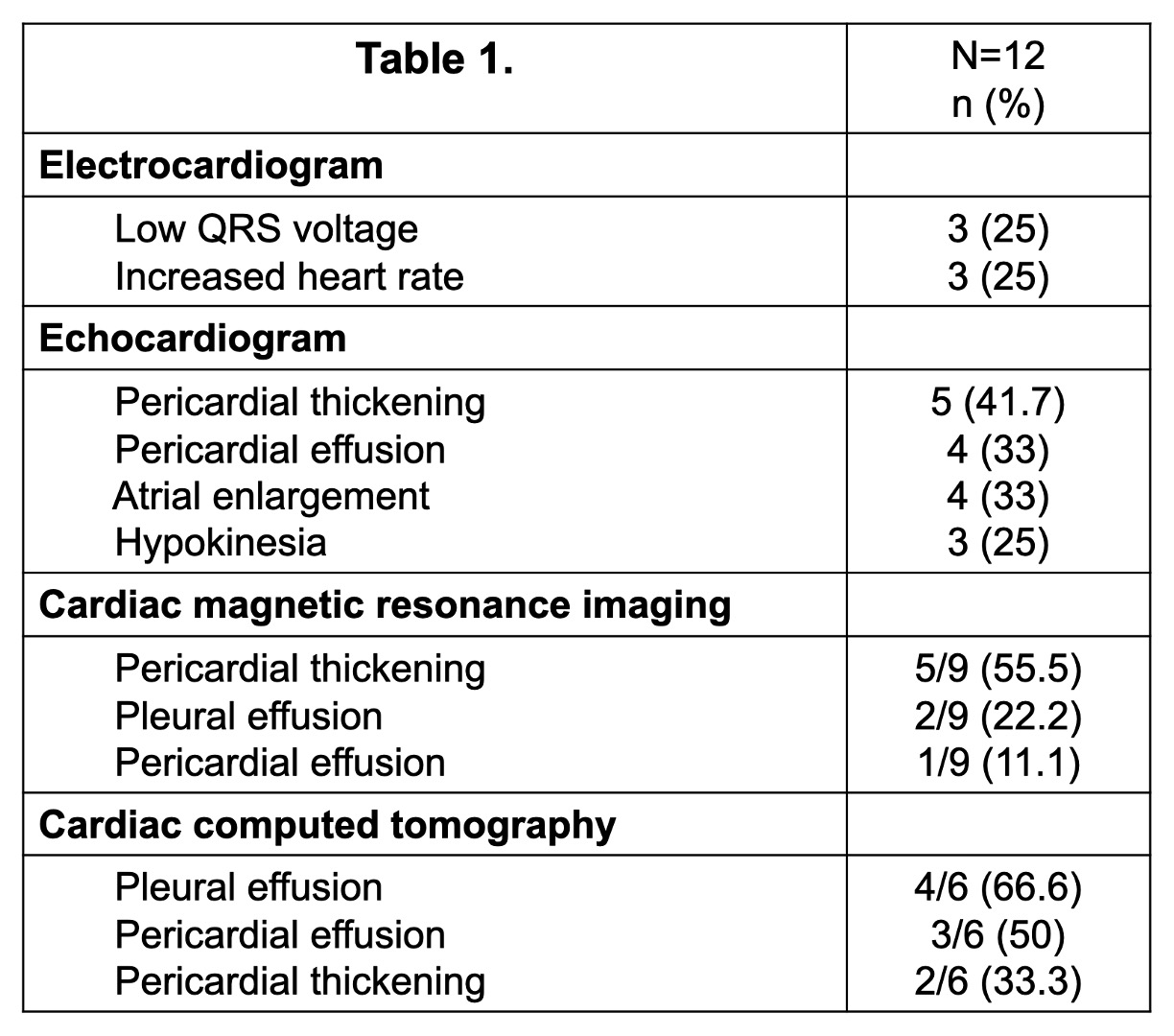
Results: Sixty-six cases were reviewed, of which 10 had an identified etiology. Of the remaining 56, only 12 had a pericardial biopsy. All had been classified as idiopathic (Figure 1). Mean age of 43.5 ± 14.4 years; 9 were men. Regarding clinical behavior, all patients presented with signs and symptoms of heart failure. Six (50%) patients presented with effusive CP and 10 (83.3%) with chronic CP (non-mutually exclusive). Findings on electrocardiogram, echocardiogram, cardiac magnetic resonance imaging and cardiac computed tomography are summarized in Table 1. All patients underwent pericardiectomy, with glucocorticoid treatment administered to only one patient. At last follow-up, 3 (25%) patients had died.
Lymphoplasmacytic infiltrate was found in all, fibrosis in eight, and storiform fibrosis in only one case. Obliterative phlebitis was not found. In 2 cases the IgG stains were not assessable, so the IgG4/IgG ratio was calculated in 10 cases. The median number of IgG4+ plasma cells/HPF was 30.5 (IQR 16.5-41). The median IgG4/IgG ratio was 59.5% (IQR 27-66). All cases had >10 IgG4+ plasma cells/HPF while 7/10 (70%) had an IgG4/IgG ratio >40%. According to the ICP, 1 (8.3%) case was highly suggestive, 6 (50%) had probable histological characteristics, and 5 (41.6%) showed insufficient histopathological evidence. Seven (58.3%) were diagnosed as probable IgG4-RD according to the CDCI, but only one patient met 2019 AECC for atypical IgG4-RD.
Conclusion: A significant proportion of pericardial biopsies from patients with idiopathic CP display findings indicative of IgG4-RD and meet at least one set of diagnostic or classification criteria. Considering the implications for treatment, IgG4-RD should be considered when evaluating patients with CP.
To cite this abstract in AMA style:
Cortez-Domínguez E, Hernandez-Molina G, Uribe-Uribe N, Lizardo-Thiebaud M, Martin-Nares E. IgG4-Related Disease as a Potencial Etiology of Idiopathic Constrictive Pericarditis [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/igg4-related-disease-as-a-potencial-etiology-of-idiopathic-constrictive-pericarditis/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/igg4-related-disease-as-a-potencial-etiology-of-idiopathic-constrictive-pericarditis/