Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: The anti-nuclear antibody (ANA test) is a sensitive screening tool used when assessing patients with possible autoimmune rheumatic diseases (ARD). Homogeneous staining positivity is associated with anti-ds-DNA antibodies. Logically a patient with a positive ds-DNA test would also be ANA positive. However, on occasion the ANA is negative when the anti-dsDNA antibody is positive, usually by enzyme-linked immunoassay (ELISA). The frequency with which this situation arises and whether it is more common in patients with ARDs or other conditions is not established. We performed an audit of patients tested in our clinical immunology laboratory who came into this category.
Methods: ANA was assessed by immunofluorescence on HEp-2 cells with an IgG conjugate screened at 1:80. IgG anti-dsDNA was assessed by ELISA on the Phadia 2500 analyzer Thermofisher. Positive results are reported as >/= 10 IU/ml. The ANA-negative/ dsDNA antibody-positive patients were retrospectively reviewed from the hospital’s electronic records in term of clinical and demographic features. Serologically, we also noted anti-extractable nuclear antigens (ENA and antiphospholipid (aPL) antibody positivity and complement decrease during the diagnostic phase.
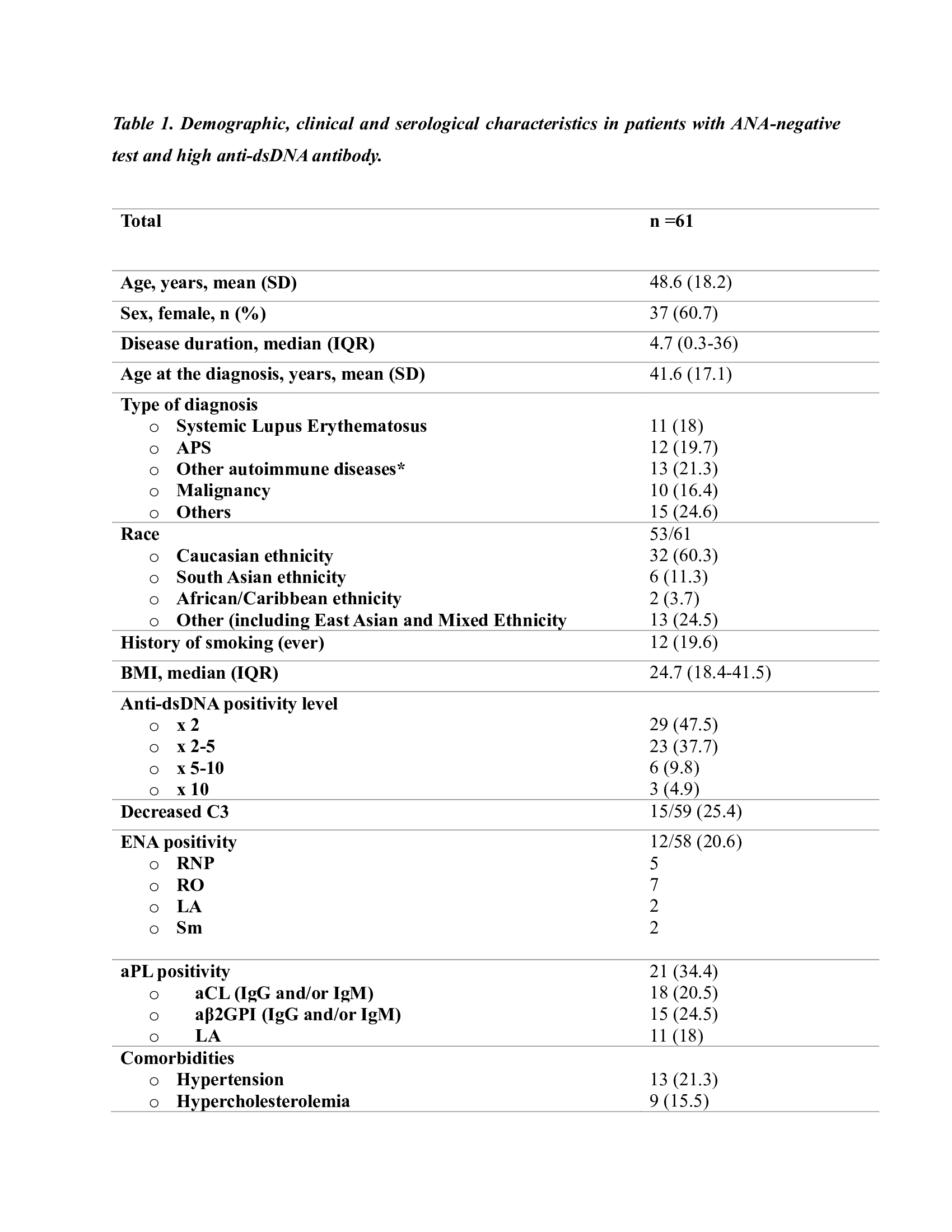
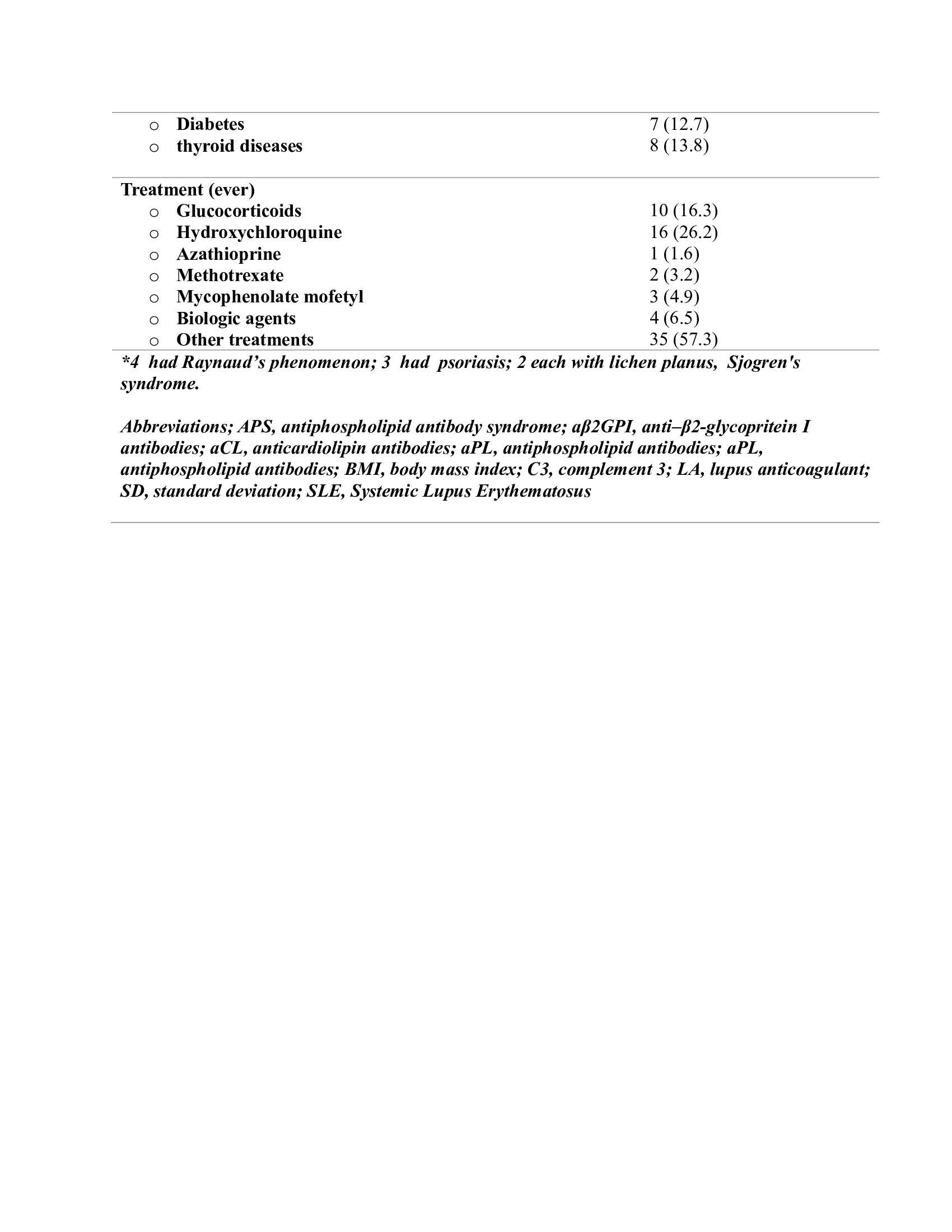
Results: 1859 samples were tested for both ANA and dsDNA antibodies. 67 (3.6%) patients were ANA negative /anti-dsDNA antibody positive. Six patients were excluded from the study due to missing data and/or positive ANA test on repeated measurements. In the remaining 61 patients, the mean age was 48.6 years (±18.2), and 37 (60.7%) were female. 21 (34.4%) patients had at least one aPL and 12/58 (20.6%) were anti-ENA positive. The most common diagnosis was the primary anti-phospholipid antibody syndrome (APS) (20.7%)11 patients had systemic lupus erythematosus (SLE) (18%), there was no difference between SLE and non-SLE patients in terms of anti-dsDNA levels (p=0.47). Ten patients had malignancy (16.4%); 4 solid organ tumours (2 patients had lung cancer, 1 each had primary tonsillar malignant neoplasm and metastatic malignant melanoma) and 6 had hematological malignancies (3 patients non-Hodgkin lymphoma and 1 patient each had Hodgkin’s lymphoma, chronic lymphocytic leukemia and low-grade T cell lymphoma) (Table 1).
Conclusion: More than 50% of ANA-negative/anti-dsDNA antibody positive patients had an ARD. The majority had APS (20%) or SLE (18%). In addition, anti-ds-DNA antibody positivity may occur in patients with malignant diseases including hematological malignancies. It is important to consider whether a malignancy might be present where fever, rash, weight loss or lymphadenopathy may cause clinical confusion. The reactive DNA sites for those antibodies may perhaps be fully covered by histones and other proteins in chromatin within nuclei in the ANA test. It might be worth testing those sera with isolated chromatin and with complexes formed in vitro by isolated DNA and histones. ANA-negative/anti ds-DNA-positive patients remain something of an enigma. Different antigens and assays may clarify the targets of the antibodies in their sera, and help determine any clinical significance in these patients.
To cite this abstract in AMA style:
Sandal Uzun G, Apsley E, Isenberg D. Identification of Patients with ANA Negative and Double Stranded DNA Positive: What Is the Significance in Daily Rheumatology Practise [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/identification-of-patients-with-ana-negative-and-double-stranded-dna-positive-what-is-the-significance-in-daily-rheumatology-practise/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/identification-of-patients-with-ana-negative-and-double-stranded-dna-positive-what-is-the-significance-in-daily-rheumatology-practise/