Session Information
Session Type: Abstract Session
Session Time: 2:00PM-2:15PM
Background/Purpose: Hand osteoarthritis (OA) is an heterogenous disease in terms of risk factors, localization and severity. This heterogeneity also applies to the clinical presentation and to the symptoms and is still poorly investigated. Our objective was to delineate the symptom-based phenotypes in a hand OA population using integrative analyses based on the cardinal symptoms of hand OA (pain, functional limitation, stiffness, esthetic discomfort).
Methods: We used the baseline data from the hospital-based hand OA cohort DIGICOD (PMID: 33689840). Clustering segregation was performed on AUSCAN subscores (0-100) of pain, function, stiffness separately, and the visual analog scale (0-100 mm) of esthetic discomfort. Hierarchical agglomerative clustering analyses were performed on 389 patients based on the Euclidean distance and the Ward D2 agglomeration method. Differences between cluster’s characteristics were assessed by Kruskal-Wallis, Wilcoxon and Fisher exact tests. The Bonferroni method was applied on adjusted p-values to correct for multiple testing.
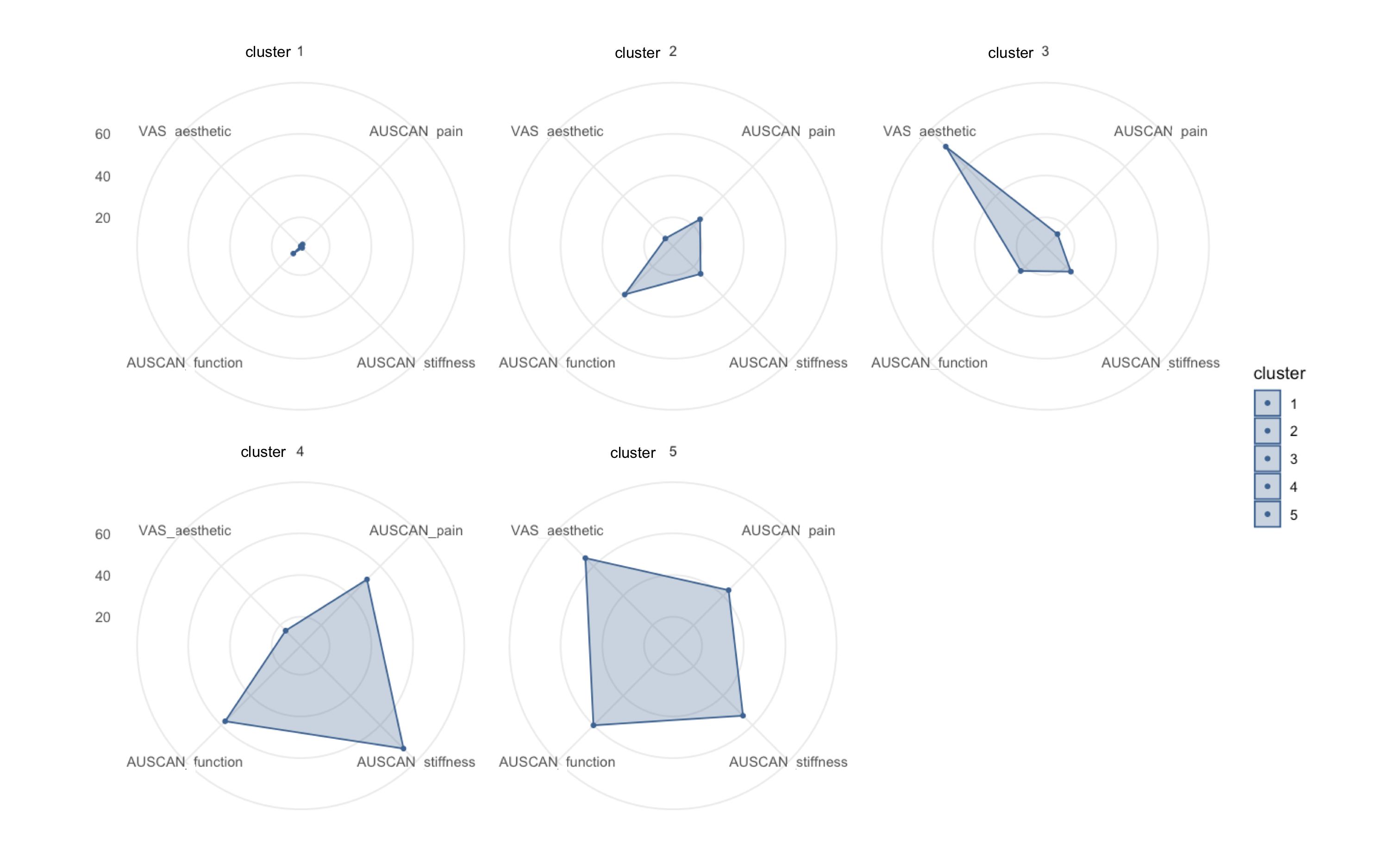
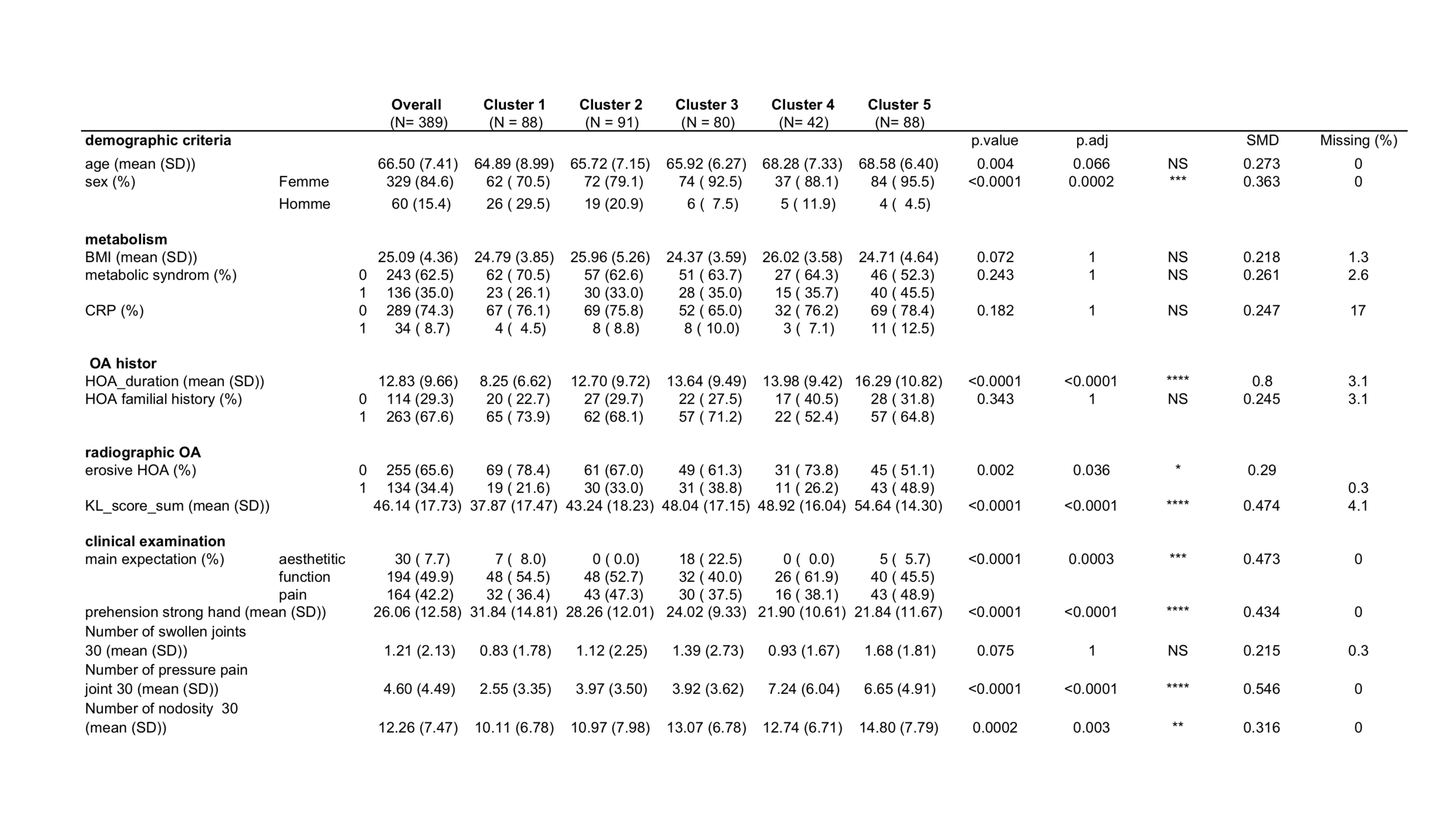
Results: Among the 389 patients analyzed, the AUSCAN subscores and the visual analog scale of esthetic discomfort enabled to identify 5 distinct clinical clusters by hierarchical clustering (Figure 1). We further characterized the composition of these clusters (Figure 2). Cluster 1 (N=88) is mainly composed of low symptomatic patients, cluster 2 (N = 91) of patients with mild symptoms (pain, stiffness and functional limitation), cluster 3 (N=80) of patients displaying esthetic discomfort mainly (without pain), cluster 4 (N =42) of high level of pain, stiffness and functional disability but without esthetic discomfort and cluster 5 (N=88) of the combined features of cluster 4 plus high level of esthetic discomfort. Age and hand OA duration were significantly different amongst clusters and higher in clusters 4 and 5 (p=0.06 and p=0.0002). Men were mostly present in low and mild-symptomatic cluster 1 and 2 (p=0.002). The clusters did not differ significantly for BMI, metabolic syndrome and CRP level, although metabolic syndrome represented 45.4 % of the highly symptomatic cluster 5 vs 26.1 % of low symptomatic cluster 1 (p= 0.01). The esthetic discomfort (corresponding to clusters 3 and 4) was associated with higher number of articular nodes (p=0.0003) and with radiographic erosive hand OA (p=0.04). Clusters 3, 4 and 5 were composed with patients more severe joint structure alteration since they displayed higher sum of the Kellgren Lawrence score for all hand joints (p< 0.00001) compared to cluster 1. Clusters 4 and 5 have also a higher Hospital Anxiety and Depression score (p=0.0004). Patients’ main expectation of improvement in all clusters was function, except pain for the highly symptomatic cluster 5. Only cluster 4 and 5 which represented one third of our cohort (N=130) had a mean AUSCAN pain score ≥ 40 mm.
Conclusion: The identification of these 5 clinical symptomatic phenotypes through hierarchical clustering illustrates the heterogeneity of the clinical presentation of hand OA. This opens toward a tailored therapeutic management according to each cluster and may help rationalizing patient recruitment in clinical trials evaluating symptomatic drugs.

To cite this abstract in AMA style:
Binvignat M, Pires G, Tchitchek N, Courties A, Costantino F, Klatzmann D, Combe B, Dougados M, Richette P, Mariotti-Ferrandiz E, Berenbaum F, Sellam J. Identification of Clinical Phenotypes of Hand Osteoarthritis Using Hierarchical Clustering Method [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/identification-of-clinical-phenotypes-of-hand-osteoarthritis-using-hierarchical-clustering-method/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/identification-of-clinical-phenotypes-of-hand-osteoarthritis-using-hierarchical-clustering-method/