Session Information
Session Type: Poster Session C
Session Time: 1:00PM-3:00PM
Background/Purpose: Post-visit discharge instructions (DCI) are an important supplement to the patient visit that serves to reinforce a patient’s understanding of their diagnosis, medications and treatment plan. They empower patients, improve compliance, and promote health literacy. DCI are especially important in the care of rheumatology patients given the chronic nature of rheumatologic diseases, co-morbidities and the side effect profiles of rheumatologic medications. As one-third of US adults have limited health literacy, it is important that DCI are easy to read and comprehend. The American Medical Association and the National Institute of Health have recommended that medical information be written at a 6th grade level. We aimed to assess the prevalence, quality, and appropriateness of DCI in an outpatient academic rheumatology clinic.
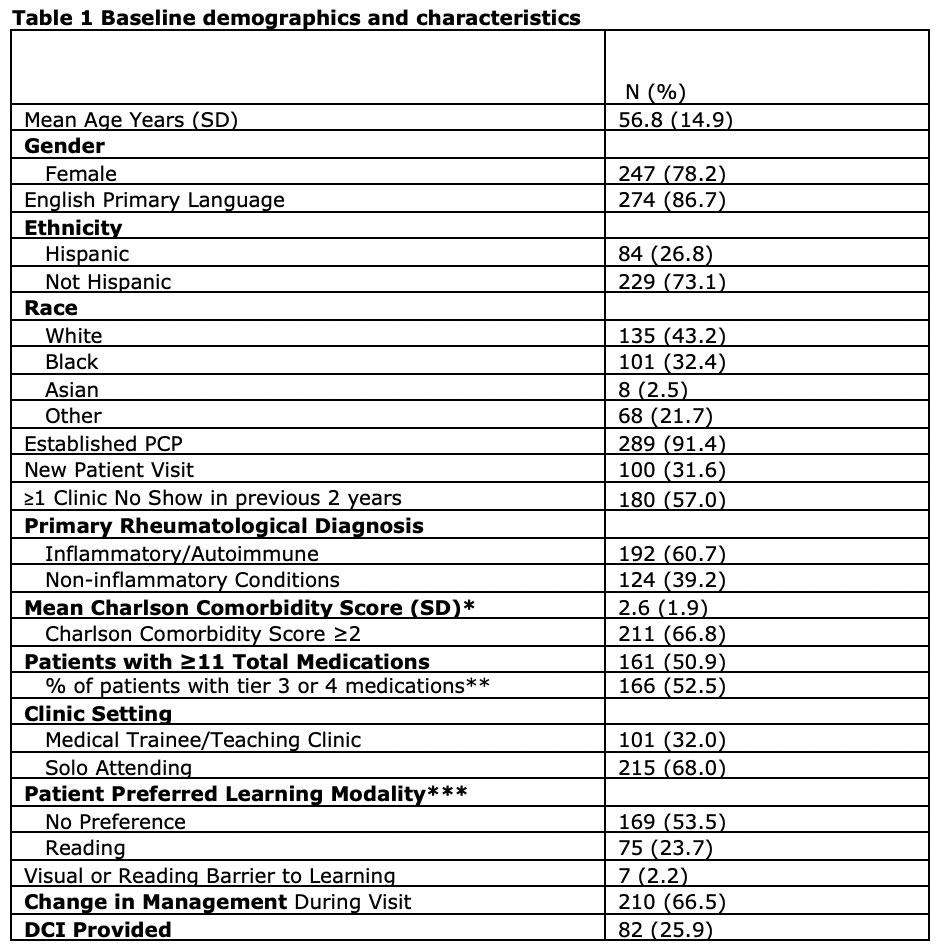
Methods: This retrospective chart review assessed all Rheumatology clinic appointments of patients ≥18 years from October 1-8, 2021. Data collected included: demographics, rheumatologic diagnoses, medications, co-morbidities, presence of DCI (Yes/No), readability of DCI (Flesch-Kincaid scores), presence of pertinent information within DCI (diagnosis, medications, management plan), type of clinic (Trainee or not) and the patients documented preferences for learning. Rheumatologic medications were stratified into 4 tiers based on their side effect profile, need for monitoring, and infection risk (Highest tier denoted greatest risk).
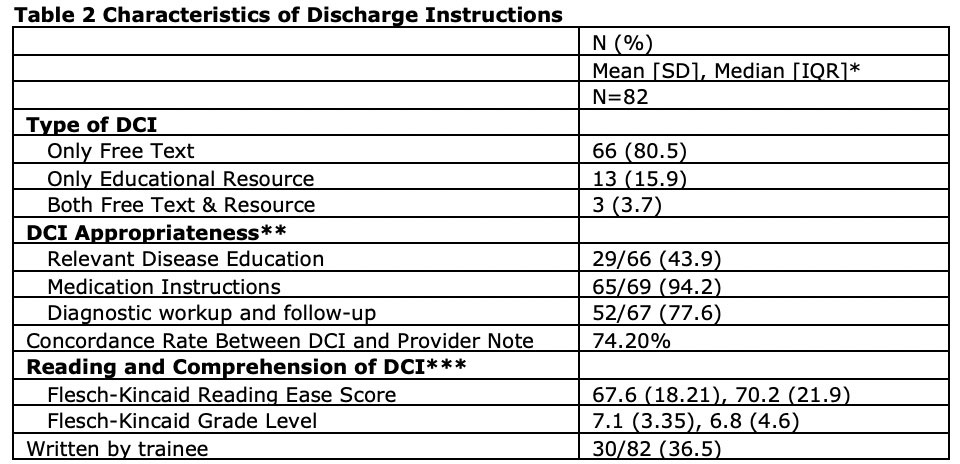
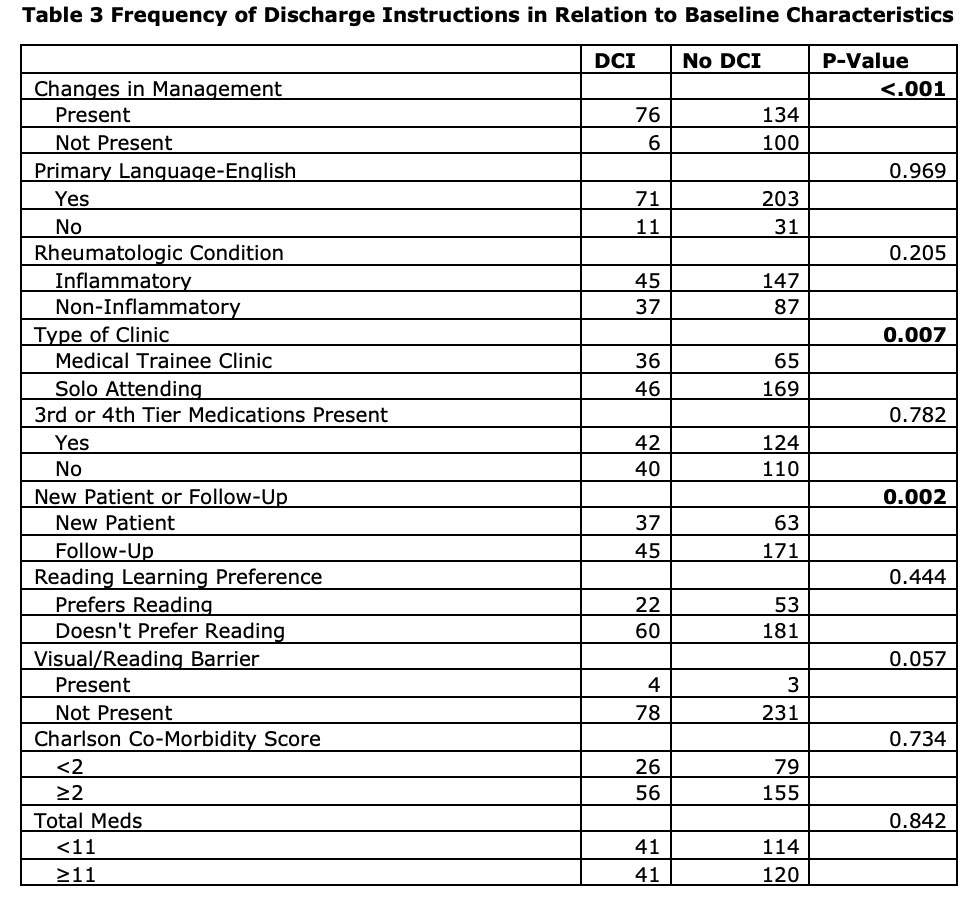
Results: Overall 82/316 patients (25.9%) received a DCI. Of the 210 (66.5%) patients with some change in management, 76 (36.1%) received DCI. Majority were provided free text instructions (80%), followed by educational resource (15.9%), and both (3.7%) (Table 1). Of the patients that received DCI, 74.2% of the instructions were concordant with the changes outlined in the providers note. The most concordant category was medication changes while the least concordant was relevant disease education. The median Flesch-Kincaid Grade Level of DCI was 6.8. (Table 2). Higher frequency of DCI use was noted with a change in management (p< 0.001), new patient visit (p 0.002), and medical trainee/teaching clinic (p 0.007). There were no differences in DCI frequency based on primary language, type of rheumatologic condition, presence of 3rd/4th tier or number of medications, comorbidities, or learning preferences/barriers. (Table 3).
Conclusion: DCI are underutilized in the rheumatology clinic. Surprisingly, patients at higher risk for worse outcomes (e.g. more comorbidities, higher number/and tier of medications used) did not translate to a greater use of DCI. When provided, DCI were at 7th grade reading level. Learning preferences and barriers while documented, were not considered when providing DCI. With the practice gaps identified, future studies to implement simple and standardized DCI is planned.
** Tiers of medications based on side effects, drug monitoring, and infection risk with higher tiers conferring higher risk
*** Learning modalities recorded in RUMC Rheumatology Clinic electronic medical record
** These 3 categories were identified by the investigators from the providers note and then compared to the DCI
*** Flesch-Kincaid tests are readability assessments that are widely used to evaluate the reading ease and grade level of a given text. The higher the reading ease score the easier the text is to understand.
To cite this abstract in AMA style:
Joseph D, Asthana A, Hassan S, Jolly M. How Often Do We Provide Relevant and Patient Centric Discharge Instructions in Rheumatology? A Single Academic Center Clinic Experience [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/how-often-do-we-provide-relevant-and-patient-centric-discharge-instructions-in-rheumatology-a-single-academic-center-clinic-experience/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/how-often-do-we-provide-relevant-and-patient-centric-discharge-instructions-in-rheumatology-a-single-academic-center-clinic-experience/