Session Information
Date: Wednesday, October 29, 2025
Title: Abstracts: Pediatric Rheumatology – Clinical III (2675–2680)
Session Type: Abstract Session
Session Time: 12:45PM-1:00PM
Background/Purpose: Timely diagnosis of Juvenile Idiopathic Arthritis (JIA) enables early initiation of therapy and improves outcomes, yet JIA patients often experience circuitous pathways to diagnosis. We aimed to characterize the healthcare utilization in the year preceding JIA diagnosis.
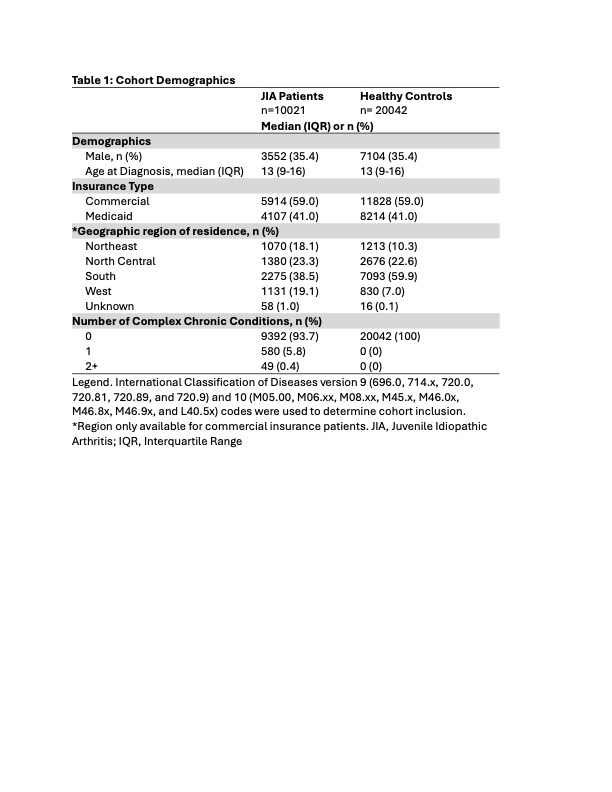
Methods: We used deidentified administrative data from the Truven Marketscan commercial and Medicaid databases (2014 to 2022). Inclusion criteria for the study were: (1) age 1-17 years and (2) diagnosis of JIA as defined by (a) ≥2 International Classification of Disease (ICD)-9 or 10 JIA codes within 6 months, (b) ≥1 JIA code from a rheumatologist, or (c) ≥1 JIA code with a claim for a JIA directed therapy or intraarticular steroid injection within 6 months. Patients were excluded if they did not have continuous enrollment in the database for 12 months prior to the index date or if they had a claim with a JIA code during that period. Age- and sex-matched controls were identified at a 2:1 ratio. The index date for JIA patients was defined as the date of the first JIA code. The index date for controls was defined as the date of a visit occurring within two months of the index date of the matched JIA patient. Healthcare utilization was defined as any inpatient admission, emergency department or urgent care visit, and outpatient claim for a billing visit with a physician or advanced practice provider. Incidence rate ratios (IRRs) were calculated to compare healthcare between JIA patients and controls in the 12 months prior to the index date, and the manual Wald test was used to calculate the relevant p-values.
Results: 10,021 children, ages 1-18 years, had an incident diagnosis of JIA in the years of study. Median age in both JIA patients and controls was 13 (interquartile range 9-16), and there was no significant difference in insurance type or prevalence of chronic conditions between the JIA patients and controls (Table 1). Healthcare utilization in the year preceding the index date was significantly higher for JIA patients versus controls (p < 0.001). JIA patients had a median of 10 healthcare encounters (interquartile range [IQR] 5 to 17) while controls had a median of 3 visits (IQR 1 to 7). This increased utilization was consistent for outpatient (IRR 2.56, p < 0.001), inpatient (IRR 4.48, p < 0.001), and emergency room/urgent care encounters (IRR 2.42, p < 0.001) (Table 2). Healthcare utilization for JIA patients escalated as the index date approached (Figure 1). JIA outpatient encounters were most frequent with generalists (74.8% of visits) and orthopedists (4.9%) in the pre-diagnosis period. Further, 22.9% of children with JIA saw an orthopedist in the year preceding JIA diagnosis, with most receiving non-specific diagnosis codes for joint pain or effusion.
Conclusion: Children with JIA have significantly higher health care utilization in comparison to age- and sex- matched healthy peers in the 12 months preceding JIA diagnosis. This pattern suggests that there may be opportunities, particularly in primary care and orthopedics, to identify JIA earlier. Understanding the patterns of utilization could help target interventions to improve the time to diagnosis, and ultimately the experiences and outcomes, for these patients.
.jpg)
.jpg)
To cite this abstract in AMA style:
Costello A, Xiao R, Jazayeri J, Brandon T, Zhang X, Rasooly I, Weiss P. High Health Care Utilization Preceding Diagnosis of Juvenile Idiopathic Arthritis [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/high-health-care-utilization-preceding-diagnosis-of-juvenile-idiopathic-arthritis/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/high-health-care-utilization-preceding-diagnosis-of-juvenile-idiopathic-arthritis/