Session Information
Session Type: Abstract Session
Session Time: 8:00AM-9:00AM
Background/Purpose: Few tools are available to evaluate the immune dysregulation in patients with severe autoimmune or inflammatory conditions that do not conform to well-defined rheumatologic diseases. The ability to identify features of the aberrant immune response in patients with undiagnosed inflammatory conditions may reveal underlying etiology and guide therapy.
Methods: We used mass cytometry to study the immune dysregulation in patients with severe immunologic conditions evaluated in the Undiagnosed Diseases Network (UDN), a multi-center program to evaluate patients with rare conditions that defy diagnosis. We analyzed PBMCs from 16 UDN patients with inflammatory conditions plus 87 non-inflammatory controls, 24 lupus patients, and 30 rheumatoid arthritis (RA) patients as comparators using two 39-marker panels.
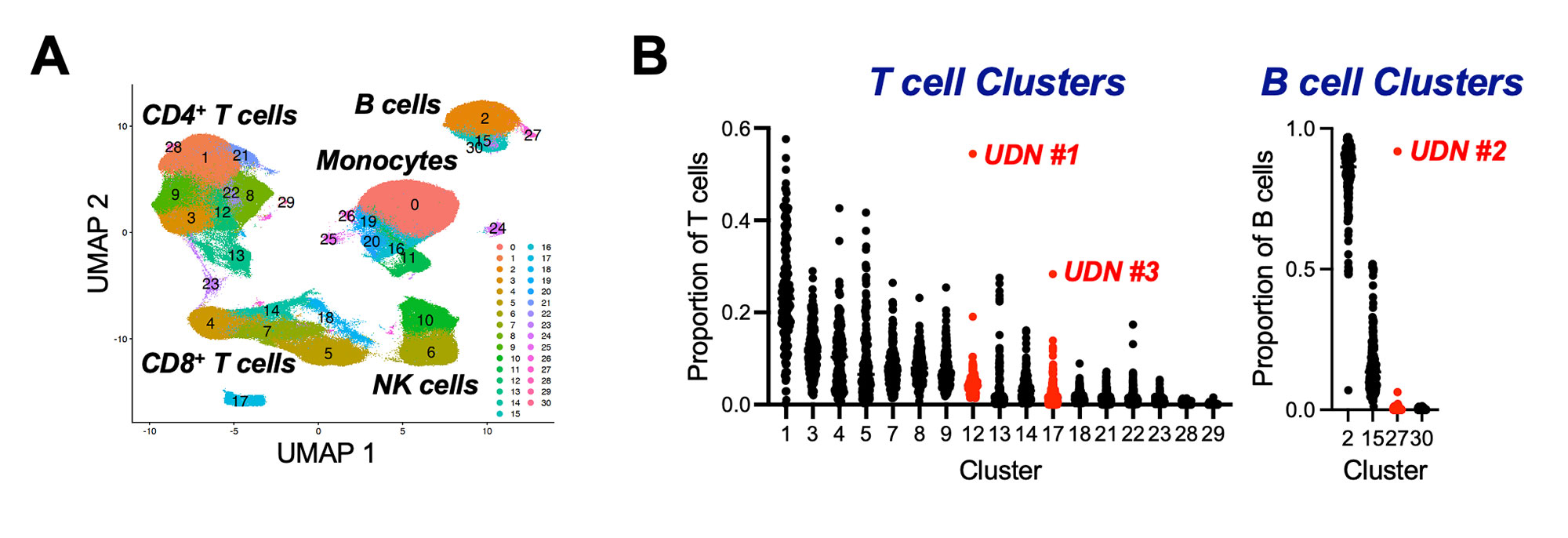
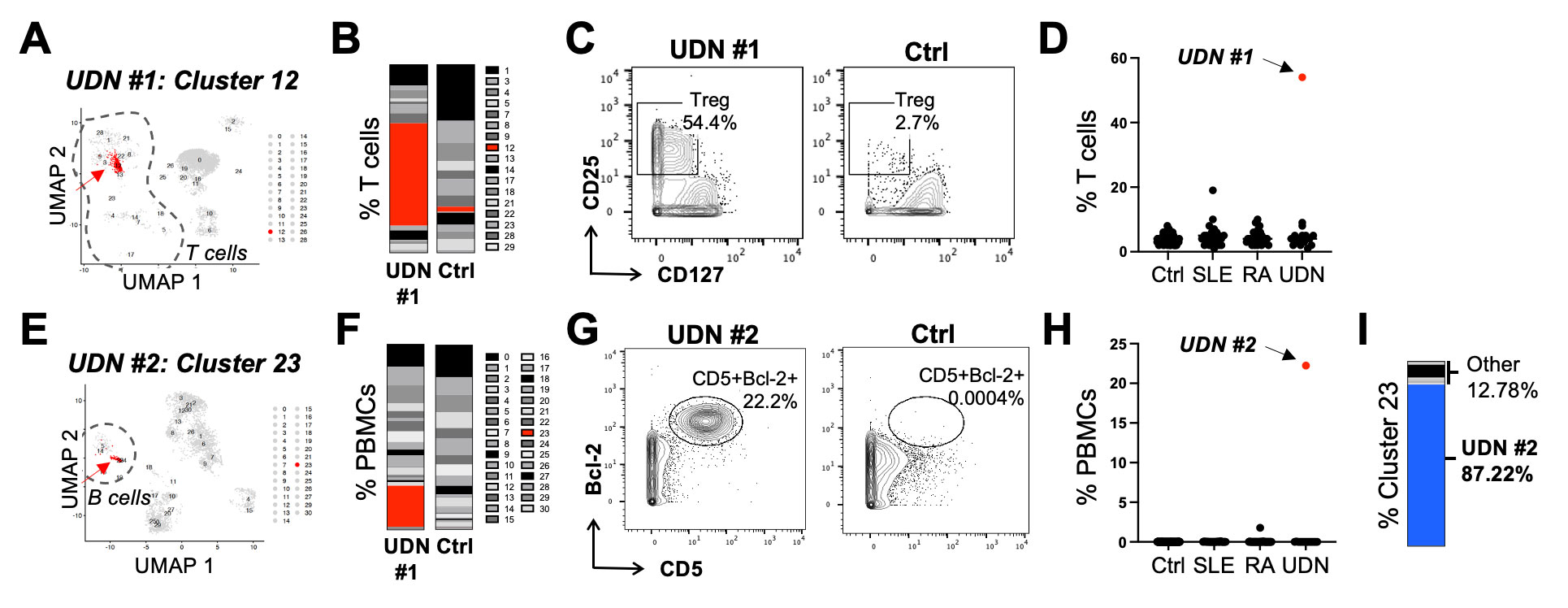
Results: Our clustering analyses of mass cytometry panels containing T or B cell-related markers revealed major cell populations and subsets (Fig. 1A). We identified patients who appeared as unique individual outliers in either of 2 types of measurements: frequency of a cluster either (1) as a proportion of total PBMCs or (2) as a proportion of T cells, B cells, or combined monocytes and natural killer cells. We defined an extreme upper outlier as a case in which the single highest patient value is >2-fold higher than the next highest patient. This simple approach identified outlier features in 5/16 UDN patients (31.3%) and in 0/121 (0.0%) of comparator patients, indicating significant enrichment of outlier features in UDN patients (p< 0.001 Fisher’s exact test) (Fig. 1B). UDN #1 is a patient with an 8-year history of debilitating global erythroderma, anhidrosis, and alopecia. We discovered that this patient had a markedly expanded population of CD25hiCD127– Tregs (Fig. 2A) comprising 54% of all T cells (average=4.7±4.5%) (Fig. 2B-D). Subsequent TCR clonality studies of blood and skin samples revealed the Treg population to be polyclonal, and T cell-directed therapies were trialed. Longitudinal single-cell RNA sequencing analyses revealed a reduction in Treg frequency with abatacept without clinical improvement, but with subsequent clinical improvement with JAK inhibitors. UDN #2 is a patient with a 4-year history of worsening cranial nerve palsies who failed multiple immunosuppressive therapies. We identified a population of CD5+Bcl-2+ B cells (Fig. 2E) comprising 22% of PBMCs (Fig. 2F-H). Strikingly, 87% of all cells in this unique cluster originated from UDN #2 (Fig. 2I). Clinical evaluation subsequently identified chronic lymphocytic leukemia and this patient was directed to oncology. Other outlier patients include: CNS disease with markedly increased Vδ2 T cells (UDN #3); progressive polyneuropathy with CD138+CD56+ expanded monocytes; and lymphadenopathy and erythema nodosum with an expanded monocyte subset.
Conclusion: High-dimensional cytometry can identify marked abnormalities in patients with inflammatory diseases that do not meet clinical criteria for rheumatic or other described disorders. Integrating cytometric analyses with clinical findings and genetic variants offers a promising approach to defining pathogenic immune mechanisms in undiagnosed patients.
To cite this abstract in AMA style:
Mueller A, Sasaki T, Keegan J, Nguyen J, Griffith A, Feig E, Horisberger A, Cao Y, Keras G, Briere L, Cobban L, Simmons D, Pallais J, Sparks J, Holers V, Network U, Sweetser D, Krier J, Loscalzo J, Lederer J, Rao D. High-Dimensional Immunophenotyping with Mass Cytometry Reveals Unique Immune Cell Aberrations in Patients with Undiagnosed Inflammatory and Autoimmune Diseases [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/high-dimensional-immunophenotyping-with-mass-cytometry-reveals-unique-immune-cell-aberrations-in-patients-with-undiagnosed-inflammatory-and-autoimmune-diseases/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/high-dimensional-immunophenotyping-with-mass-cytometry-reveals-unique-immune-cell-aberrations-in-patients-with-undiagnosed-inflammatory-and-autoimmune-diseases/