Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Rheumatoid arthritis (RA) is an autoimmune, systemic disease with a rising U.S. healthcare burden. Utilizing Global Burden of Disease (GBD) 2021 estimates, we analyzed sex, age, and state specific trends in prevalence, incidence, Disability-Adjusted Life Year (DALY), and death, including attributable smoking burden.
Methods: We performed a descriptive analysis with GBD 2021 estimates for RA in all 50 U.S. states and District of Columbia from 1990 to 2021. Age-standardized prevalence, incidence, DALY, and death rates were stratified by sex and age group. Choropleth maps were created to display geographic disparities, and box plots were employed to compare inter-state variation and gender differences. States were also grouped based on the magnitude and temporal trends of smoking-attributable RA DALY percentages.
Results: Montana, Wyoming, and New Mexico consistently ranked among the top three states for overall RA burden, with Montana showing highest age-standardized prevalence (464.73 per 100,000) and DALY rate (73.17). The District of Columbia, California, and Mississippi reported the lowest prevalence and DALY rates. RA burden increased progressively with age. The 55+ group had the highest rates across all parameters (DALY: 162.8; incidence: 46.98; prevalence: 1014.63; death: 2.16), while individuals under 20 had minimal burden (DALY: 4.44; death: 0.00).Females had consistently higher burden than males across all states and age groups. For example, Montana’s female DALY rate was 104.4 compared to 41.77 for males. Smoking-attributable RA DALY rates showed an overall national decline but remained highest in states such as Montana, Kentucky, and Wyoming, which consistently ranked in the top three from 1990 to 2021. West Virginia, Tennessee, and New Mexico remained within the top 10, highlighting regions of persistent burden. Meanwhile, states such as Colorado, Minnesota, and Nevada showed significant improvement, dropping out of the top 15. In contrast, Arkansas, Kentucky and South Dakota climbed the ranks, reflecting worsening trends in smoking-related RA burden in those regions.
Conclusion: Substantial disparities in RA burden exist across U.S. states, with consistently high rates observed in Montana, Wyoming, and Kentucky. These differences are further amplified by sex- and age-specific trends, with older adults and females bearing a disproportionate burden. While smoking-attributable RA DALY percentages have declined nationally, several states—particularly Kentucky, Arkansas, and Missouri—continue to show persistently high or worsening burden, suggesting gaps in tobacco control. Conversely, states such as Colorado and Minnesota demonstrate improving trends.These findings highlight the urgent need for state-specific, gender- and age-sensitive strategies to mitigate RA burden and address modifiable risks like smoking. Targeted interventions may include stricter tobacco control policies, tailored public health campaigns, improved telehealth access for rheumatologic care, and early screening integrated into primary care for high-risk groups. Focused, equitable efforts are critical to narrowing geographic and demographic disparities in RA outcomes across the U.S.
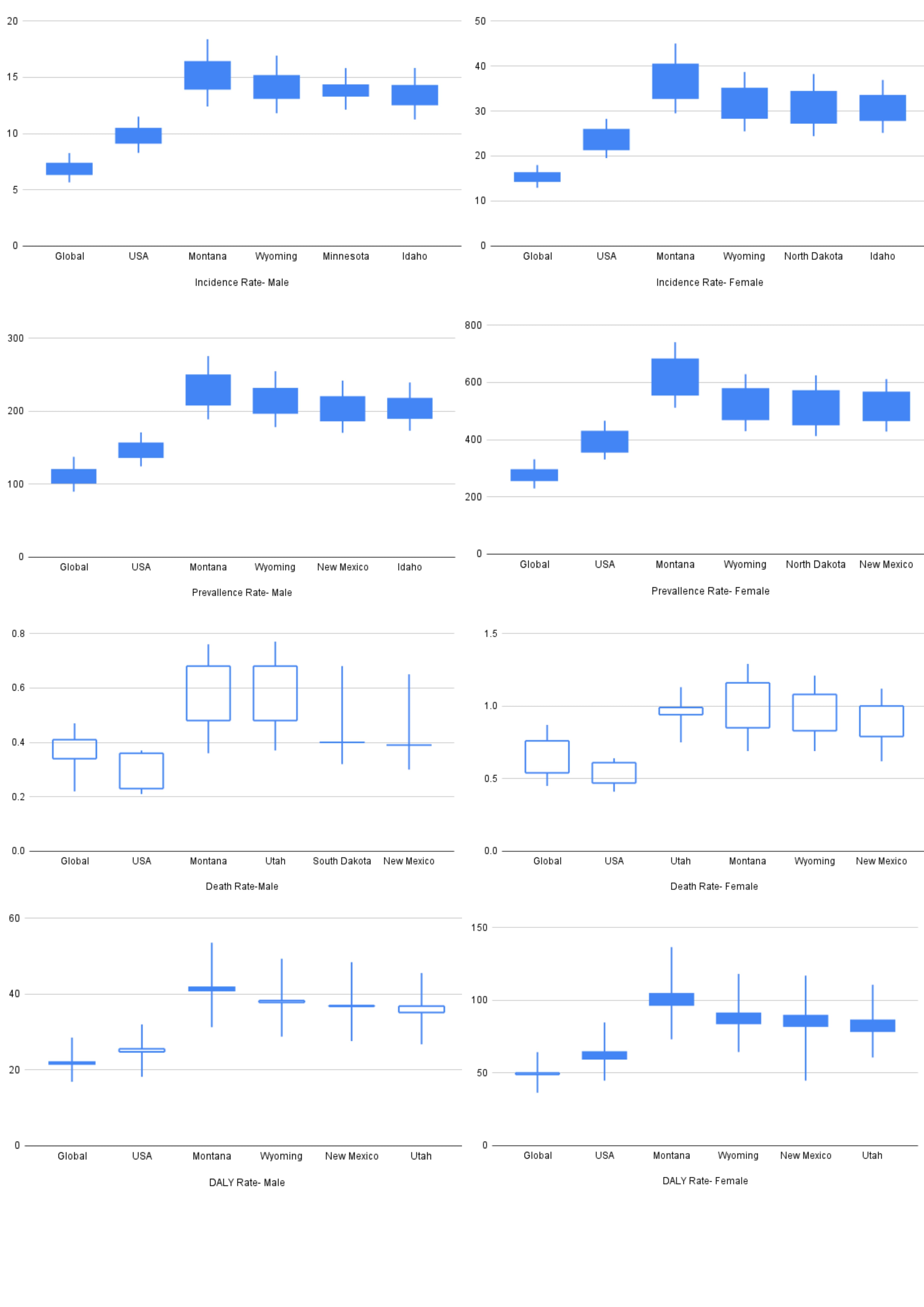 Figure 1: U.S. state-level choropleth maps showing the age-standardized burden of rheumatoid arthritis (RA) by sex.
Figure 1: U.S. state-level choropleth maps showing the age-standardized burden of rheumatoid arthritis (RA) by sex.
The top row depicts age-standardized prevalence rates in males (left) and females (right).
The bottom row shows age-standardized DALY (disability-adjusted life year) rates in males (left) and females (right).
Color gradients range from green (lower burden) to red (higher burden). Montana consistently shows the highest burden across both prevalence and DALY measures, especially among females. In contrast, states such as California and the District of Columbia demonstrate lower burden. Across all maps, females show higher RA burden compared to males, highlighting persistent sex-based disparities.
.jpg) Figure 2: Boxplots illustrating age-standardized burden of rheumatoid arthritis (RA) from 1990 to 2021 across global, U.S., and high-burden states by sex and metric. The plots compare male (left column) and female (right column) data across six domains: incidence rate, prevalence rate, death rate, and DALY rate.
Figure 2: Boxplots illustrating age-standardized burden of rheumatoid arthritis (RA) from 1990 to 2021 across global, U.S., and high-burden states by sex and metric. The plots compare male (left column) and female (right column) data across six domains: incidence rate, prevalence rate, death rate, and DALY rate.
Each box represents the interquartile range (IQR) of the metric, with the filled boxes indicating an increase and unfilled boxes indicating a decrease between 1990 and 2021. The central vertical whisker spans the widest confidence interval limits (i.e., from the lowest lower bound to the highest upper bound of both years), indicating the maximum possible uncertainty range over time.
The x-axis includes Global, USA, and the top four high-burden U.S. states identified for each metric. Notably, Montana and Wyoming appear consistently among the highest for most metrics, particularly in females, who show greater overall burden across incidence, prevalence, DALY, and death.
.jpg) Figure 3: Trends in the top 15 U.S. states by age-standardized DALY rate attributable to smoking-related rheumatoid arthritis (RA) from 1990 to 2021. Each column represents rankings by year (1990, 2000, 2010, 2021), with corresponding DALY rates in parentheses.
Figure 3: Trends in the top 15 U.S. states by age-standardized DALY rate attributable to smoking-related rheumatoid arthritis (RA) from 1990 to 2021. Each column represents rankings by year (1990, 2000, 2010, 2021), with corresponding DALY rates in parentheses.
Black lines indicate unchanged rank from one time point to the next.
Green lines indicate a decrease in rank (i.e., improvement/lower disease burden).
Red lines indicate an increase in rank (i.e., worsening disease burden).
Green downward arrows denote states that were ranked in the top 15 in respective time frame but dropped out by 2021.
Red upward arrows denote states that entered the top 15 in respective time frame by 2021.
This visualization reflects geographic and temporal disparities in smoking-attributable RA burden across the U.S., highlighting states with persistently high burden (e.g., Montana, Kentucky) and those showing worsening trends (e.g., Arkansas, South Dakota).
To cite this abstract in AMA style:
Chirumamilla P, Majety S, Nimmagadda R, Medarametla R, Sunkara P, Bandarupalli P, Cherukuri A, Anne H. Geographic and Demographic Patterns of Rheumatoid Arthritis in the United States: Insights from GBD 2021 [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/geographic-and-demographic-patterns-of-rheumatoid-arthritis-in-the-united-states-insights-from-gbd-2021/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/geographic-and-demographic-patterns-of-rheumatoid-arthritis-in-the-united-states-insights-from-gbd-2021/