Session Information
Session Type: Abstract Session
Session Time: 3:15PM-3:30PM
Background/Purpose: Oral NSAIDs are recommended for OA management. However, many patients with OA have contraindications to NSAIDs or have comorbidities that warrant precaution. Because few other oral therapies are available, such patients may still receive NSAIDs or may instead receive opioids, which are not recommended and have numerous concerning adverse effects. They may also receive physical therapy (PT), an effective option, as a safe alternative. We evaluated the patterns of NSAID, opioid, and PT use among persons with newly diagnosed knee or hip OA with and without NSAID contraindications or precautions using population-based Swedish register data.
Methods: We used register data on healthcare use and dispensed drugs, and population register to identify adults aged ≥35 as of Jan 1, 2010 residing in Skåne region in Sweden, between 1998-2009 and without a knee or hip OA diagnosis during this time. Among this cohort, we identified people with incident knee or hip OA using ICD-10 codes between 2010- 2015. We identified contraindications to or precautions for oral NSAIDs based on ICD-10 codes prior to or at the time of OA diagnosis. Contraindications included gastrointestinal bleed/ ulcer, chronic kidney disease (CKD) stage ≥3 (dialysis, transplant), acute renal failure. Precautions included coronary artery disease, heart failure, gastroesophageal reflux disease, inflammatory bowel disease, CKD stage 1 or 2, other kidney diseases. During the first year after a new OA diagnosis among those with vs. without contraindications or precautions, we evaluated the prevalence and relative risk of: 1) regular oral NSAID use (see Figure 1 for definition); 2) regular opioid use (see Fig 1); 3) physical therapy visit descriptively and in confounder-adjusted logistic regression models with standardization to compute risk ratios.
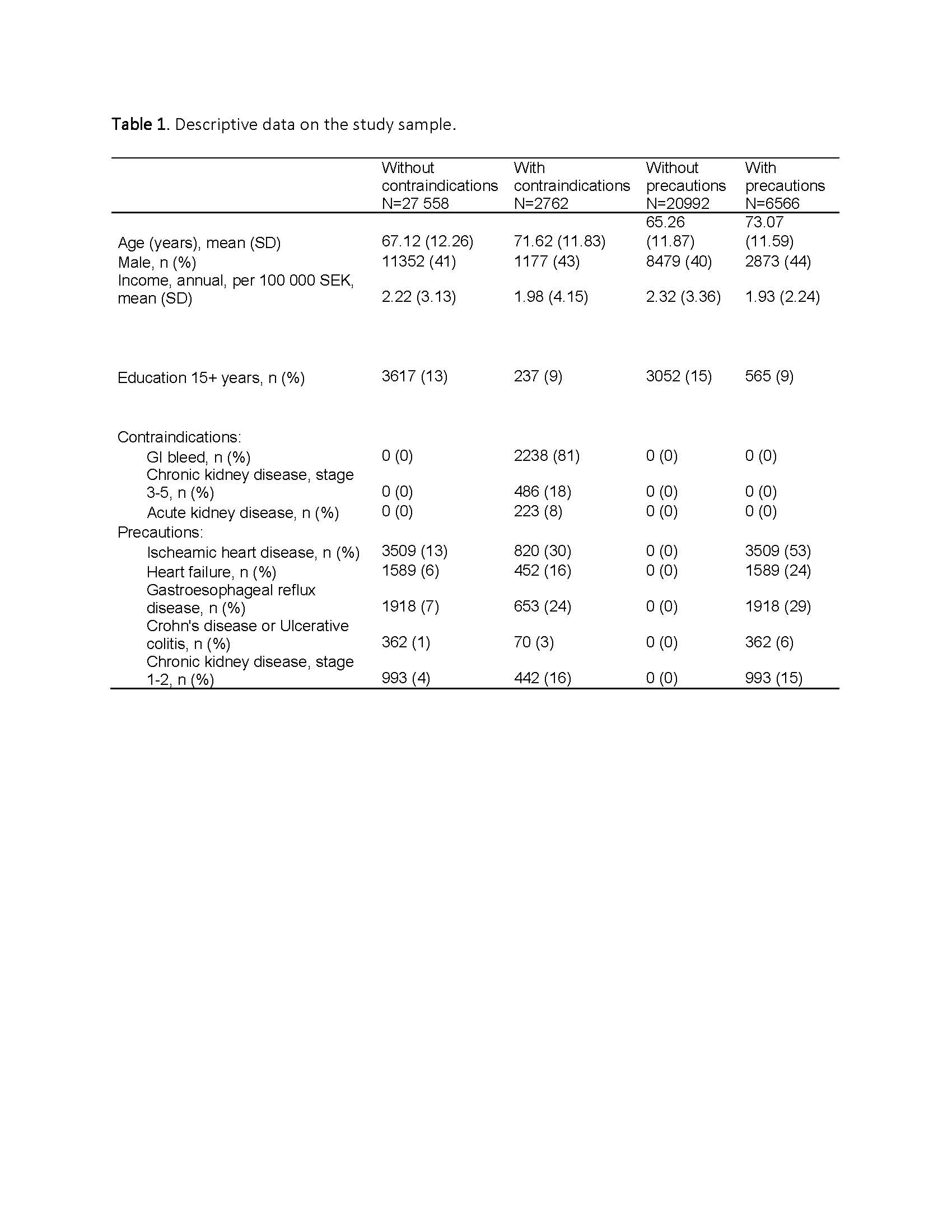
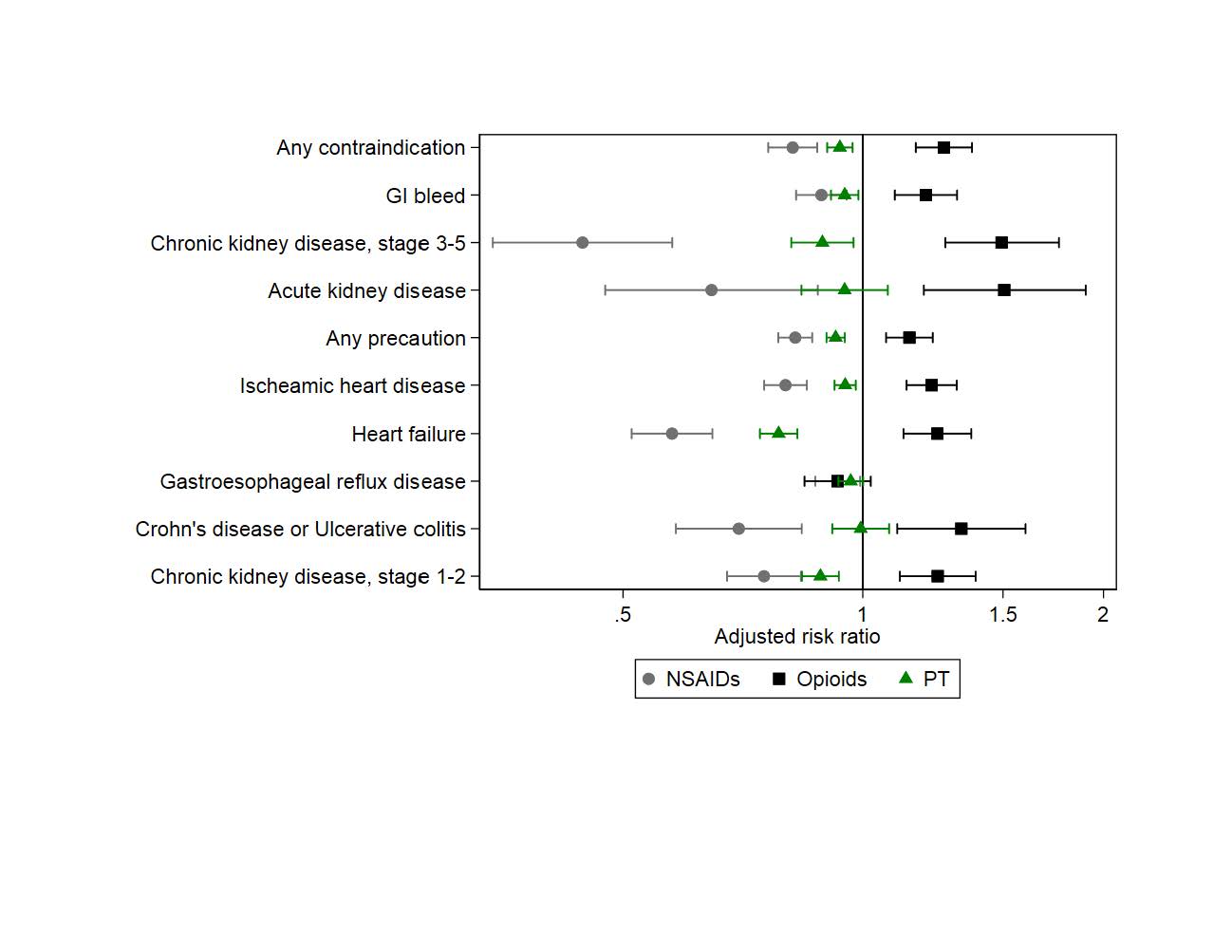
Results: We included 30,320 persons (21,682 knee OA; 9124 hip OA; 486 were diagnosed with both on the same date; mean age 67, ~41% male, Table 1). Overall, 9.1% had contraindications to NSAIDs, and 21.7% had at least one precaution. There was lower prevalence of regular NSAID use among those with vs. without contraindication to NSAIDs (22% vs. 30%), but higher prevalence of regular opioid use (21% vs. 15%) (Figure 1a); a similar pattern was seen for those with vs. without precautions for NSAIDs (NSAID use: 23% vs. 32%; (opioid use: 18% vs. 14%) (Figure 1b). The lowest prevalence of regular NSAID use was among those with CKD stage ≥3 (10%); they also had highest prevalence of regular opioid use (25%). Prevalence of PT was slightly lower among those with contraindications (51%) or precautions (50%) than those without (55% and 57%, respectively). In adjusted analyses, those with contraindications or precautions were at 1.2 to 1.5 times higher risk of regular opioid prescriptions than those without, while use of PT was not increased for any group (Figure 2).
Conclusion: People with knee or hip OA who have contraindications to or precautions for NSAIDs had higher risk of regular opioid use, but not PT, within the first year of their OA diagnosis. These data highlight the negative impact of having a paucity of treatment options for people with OA who are unable to safely use NSAIDs, and lack of sufficient use of PT for these at-risk patients.

To cite this abstract in AMA style:
Neogi T, Dell'isola A, Englund M, Turkiewicz A. Frequent Use of Prescription Oral NSAIDs Among People with Knee or Hip Osteoarthritis Despite Contraindications to or Precautions with NSAIDs [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/frequent-use-of-prescription-oral-nsaids-among-people-with-knee-or-hip-osteoarthritis-despite-contraindications-to-or-precautions-with-nsaids/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/frequent-use-of-prescription-oral-nsaids-among-people-with-knee-or-hip-osteoarthritis-despite-contraindications-to-or-precautions-with-nsaids/