Session Information
Date: Tuesday, October 28, 2025
Title: (1990–2014) Metabolic & Crystal Arthropathies – Basic & Clinical Science Poster II
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: As reported in Cell Press journals,1,2 intestinal commensal purine-degrading bacteria anaerobically degrade urate to anti-inflammatory short chain fatty acids, including butyrate, and thus may partially compensate for uricase absence in humans. This enables homeostatic control over urate levels, particularly in those with chronic kidney disease (CKD) where the role of extrarenal urate elimination increases. Indeed, in severe CKD the gut becomes predominant site of urate disposition. Since treatment with anaerobe-targeted antibiotics rapidly elevates serum and cecal urate in mice,1 and has been linked to increased incidence of gout diagnosis in a Stanford University cohort,1 we hypothesized such treatment in humans with CKD is linked to more frequent gout flares. We conducted target trial emulations to compare rate of gout flares among patients (stratified by CKD) treated with clindamycin, an antibiotic targeting both aerobic and anaerobic microbes, versus trimethoprim/sulfamethoxazole (T/S), antibiotic with limited anaerobic coverage.
Methods: We included adults aged ≥18 years with dispensed prescriptions for ≥ 5 days of oral clindamycin or T/S, and no diagnosis of gout or receipt of antibiotics in prior 12 months. Randomization was emulated based on pre-exposure prognostic factors including sociodemographics, infections, comorbidities, medications, and healthcare use. Primary outcome was gout flare counts over 3 months after index date, ascertained by emergency department, hospital, outpatient, and prescription records;3 We assessed C. difficile infection as positive control outcome and osteoarthritis (OA) encounter as negative control outcome. Poisson and Cox models were used to calculate adjusted rate ratios (RR) and hazard ratios (HR) with 95% confidence intervals (95% CI).
Results: After 1:1 matching, we included 306,058 adults initiating clindamycin and 306,058 initiating T/S (43% male, mean age 47). Baseline characteristics were well-balanced between treatment arms (standardized differences < 0.1 for all factors). Among the 13,550 propensity-matched individuals with CKD, rate of gout flares was higher among those initiating clindamycin vs T/S (37.2 vs 10.3 per 1000 person-years, respectively), with adjusted RR 3.71 (95% CI: 2.17, 6.34) (Table 1). Associations were smaller but remained significant among non-CKD, with adjusted RR 1.61 (1.37, 1.89) (Table 1) (p-interaction 0.003). Associations persisted when assessing gout flares for 12 months after index date (Table 1) and comparing rates of all gout-primary encounters, regardless of medication dispensing (Table 2). Clindamycin initiators showed higher risk of C. diff. infection vs T/S (HR 3.14 [2.02, 4.90]), but no altered risk of OA encounter, both as expected.
Conclusion: In this general population study, exposure to an anaerobe-targeted antibiotic was associated with >3-fold higher rate of gout flares versus the non-anaerobe-targeted antibiotic T/S, among those with CKD. These findings support a substantial role of gut purine-degrading bacteria (PDB) in urate disposition, as well as suppression by gut PDB of gouty inflammation, particularly in those with CKD.1. PMID 375411972. PMID 37279756 3. JAMA 2024 PMID 38319333
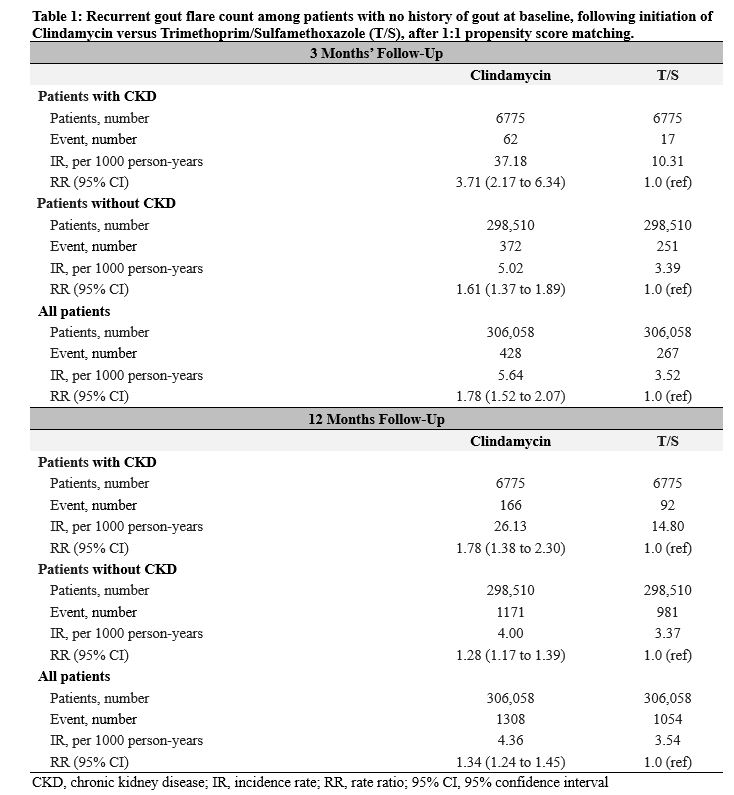 Table 1: Recurrent gout flare count among patients with no history of gout at baseline, following initiation of Clindamycin versus Trimethoprim/Sulfamethoxazole (T/S), after 1:1 propensity score matching.
Table 1: Recurrent gout flare count among patients with no history of gout at baseline, following initiation of Clindamycin versus Trimethoprim/Sulfamethoxazole (T/S), after 1:1 propensity score matching.
.jpg) Table 2: Frequency of gout-primary outpatient encounters among patients with no history of gout at baseline, following initiation of Clindamycin versus Trimethoprim/Sulfamethoxazole (T/S), after 1:1 propensity score matching, 3 months’ follow-up.
Table 2: Frequency of gout-primary outpatient encounters among patients with no history of gout at baseline, following initiation of Clindamycin versus Trimethoprim/Sulfamethoxazole (T/S), after 1:1 propensity score matching, 3 months’ follow-up.
To cite this abstract in AMA style:
McCormick N, Rai S, Yokose C, lu l, Terkeltaub R, Nazzal L, Li H, Dodd D, Choi H. Exposure to Anaerobic Antibiotics and Risk of Gout Flares: Target Trial Emulation for the Potential Role of the Gut Microbiome in Gout and Chronic Kidney Disease (CKD) [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/exposure-to-anaerobic-antibiotics-and-risk-of-gout-flares-target-trial-emulation-for-the-potential-role-of-the-gut-microbiome-in-gout-and-chronic-kidney-disease-ckd/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/exposure-to-anaerobic-antibiotics-and-risk-of-gout-flares-target-trial-emulation-for-the-potential-role-of-the-gut-microbiome-in-gout-and-chronic-kidney-disease-ckd/