Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Juvenile idiopathic arthritis (JIA) is a chronic autoimmune disease complicated by significant morbidity and disability with suboptimal rates of prolonged remission, decreased health-related quality of life, and functional limitations. The Pediatric Rheumatology Care and Outcomes Improvement Network (PR-COIN) is a 23-site North American pediatric rheumatology learning health network with a focus on improving outcomes in patients with JIA. PR-COIN has a centralized patient registry with over 13,500 registered patients and over 89,000 visits of patients with JIA to track outcome and process measures. We aimed to assess for health disparities in our collaborative JIA population by evaluating our performance on disease activity outcomes, overall wellbeing, and pain by race, ethnicity, age, sex assigned at birth, and JIA subtype.
Methods: We performed a retrospective analysis of all patients registered in the PR-COIN registry with at least one visit from April 2011 to March 2024 with patient data from 18 children’s hospitals. If patients had more than one visit in the registry, we selected the data from the most recent visit. We calculated the follow-up length of the latest visit to the diagnosis date and excluded patients with a disease duration of less than 6 months. We then conducted a cross-sectional analysis to estimate the association between race-ethnicity groups and health outcomes including physician global assessment of disease activity score, patient/parent global assessment of overall well-being score, active joint count, 10-joint clinical Juvenile Arthritis Disease Activity Score (cJADAS10), and arthritis-related pain score.
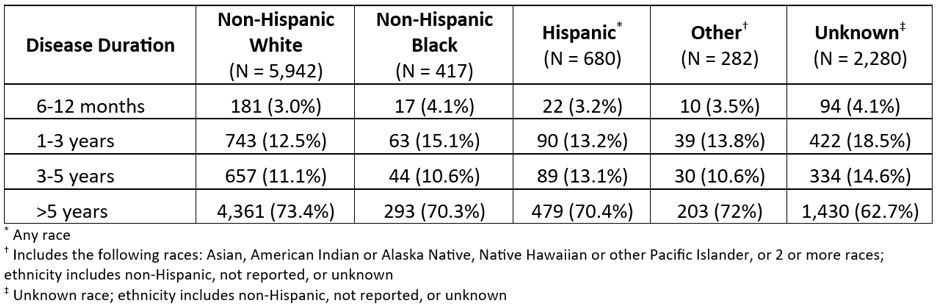
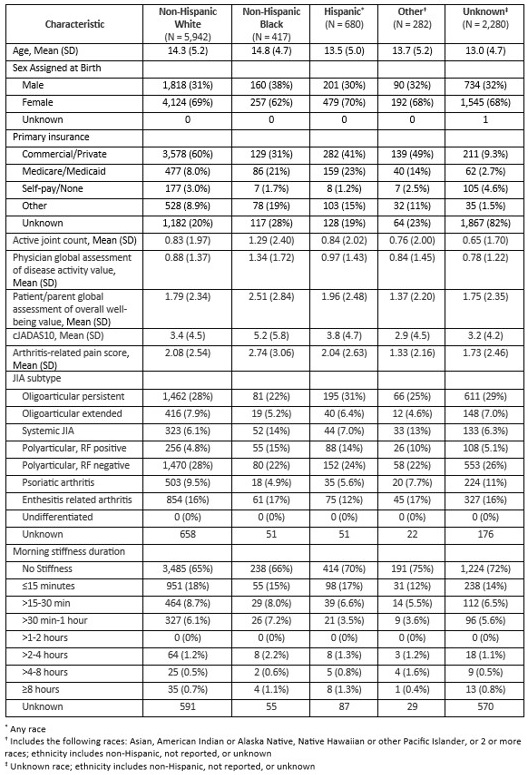
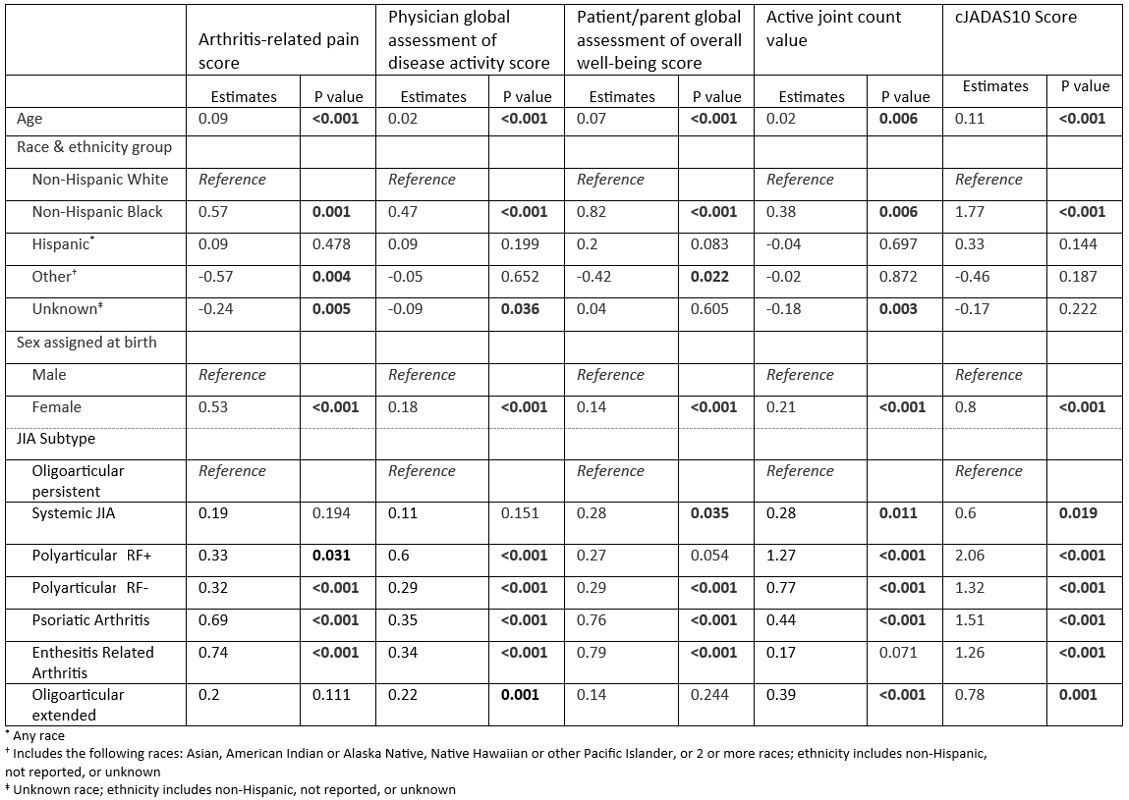
Results: Data from 9,601 patients were analyzed. 61.9% of patients with JIA identified as non-Hispanic White, 4.3% as Black or African American, 7.1% as Hispanic, 2.9% as Other, and 23.7% were unknown (Table 1). Table 2 highlights demographic and disease characteristics by race and ethnicity group. When controlling for race/ethnicity, sex assigned at birth, and JIA subtype, age was positively and significantly associated with higher scores of arthritis-related pain, physician global assessment of disease activity, patient/parent global assessment of overall well-being, active joint count, and cJADAS10 (Table 3). Non-Hispanic Black patients with JIA had statistically higher cJADAS10 scores compared to non-Hispanic Whites, in addition to statistically higher arthritis-related pain scores, physician global assessment of disease activity values, patient/parent global assessment of overall well-being scores, and active joint count values. Females had statistically higher scores compared to males for all outcome variables assessed. Furthermore, when compared to patients with the oligoarticular persistent JIA subtype, patients with polyarticular and psoriatic subtypes had significantly higher scores for pain, overall wellbeing, and disease activity outcomes.
Conclusion: We found disparities in outcomes of patients with JIA related to race, sex, and age. This information is imperative to drive further improvement efforts and enhance care coordination to close disparity gaps and improve outcomes for all patients with JIA.
To cite this abstract in AMA style:
Harris J, Singleton J, Vora S. Evaluation of Health Disparities in Outcomes of Patients with Juvenile Idiopathic Arthritis [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/evaluation-of-health-disparities-in-outcomes-of-patients-with-juvenile-idiopathic-arthritis/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/evaluation-of-health-disparities-in-outcomes-of-patients-with-juvenile-idiopathic-arthritis/