Session Information
Date: Sunday, November 13, 2022
Title: Spondyloarthritis Including PsA – Diagnosis, Manifestations, and Outcomes Poster III
Session Type: Poster Session C
Session Time: 1:00PM-3:00PM
Background/Purpose: The enthesitis can be the earliest/primary inflammatory event in psoriatic arthritis (PsA). Clinically most of the entheses are not accessible and can’t be assessed; also can’t be differentiated from mechanical strain. The Total Body (TB)-PET/CT imaging with the 18F-FDG radiotracer captures glucose metabolism across the whole body. Thus identifies and provides a quantitative standardized measures as surrogates for the degree of systemic inflammation such as SUVmax. The objective of this study was to apply high-sensitivity TB 18F-FDG PET/CT imaging to characterize enthesitis and to determine the enthesitis burden in patients with PsA.
Methods: We prospectively recruited 20 untreated PsA patients (15 male,5 female; mean age of 56.8±16.3 years). All subjects underwent full rheumatological evaluation including Leeds enthesitis index (LEI) and a single-timepoint TB-PET/CT using 1/5th the standard radioisotope dose. 38 entheses per participant, so in 20 patients (38×20=760) were assessed. The evaluated entheses were derived from 6 different enthesitis outcome measures (LEI, San Francisco, MASES, MAJOR, SPARCC, and 4-Point enthesitis measures). Each enthesis was visually evaluated based on FDG uptake intensity using an ordinal score from 0 to 3 and quantitatively based on the maximum standardized uptake value ratio after correction to the background level (rSUVmax).
Results: Inflammation of enthesis per PET imaging was found in all subjects (n=20, 100%). Our findings suggest marked inflammation in entheses, and adjacent bone along with nail matrix inflammation in the DIP joints of PsA patients compared to OA (n=20) (Fig 1).
Here we are reporting extracted data on 15 patients. PET/CT was positive in 127 out of 543 evaluable enthesis (23.4%) in among 15 participants (average: 8.5 positive entheses per participant). The anatomical distribution of positive entheses is presented in Fig 2-A.
On clinical rheumatologic examination and PET/CT, respectively, 7 and 21 out of 82 evaluable LEI entheses were positive. PET/CT was positive in 5/7 tender entheses and detected inflammation in additional 16 LEI entheses (Fig 2-B).
SPARCC and San Francisco measures demonstrated the highest absolute number of positive entheses (66 and 59, respectively). However, components of LEI were, on average, the most metabolically active (Fig 3) with average summed rSUVmax of 14.1±9.8 compared to 8.0±5.1and 7.0±4.8 for SPARCC and San Francisco measures, respectively.
Conclusion:
1. Enthesitis likely to be a dominant pathology in PsA. TB-PET/CT scans were able to detect inflammation in significantly higher number of entheses ( >20%) when compared to rheumatologic examination of a specific clinical measure.
2. Our findings provides direct in-vivo evidence suggesting that the pathologic events in the DIP joints are largely entheseal based. We are generating data on larger patient population and expecting to substantiate this observation which will provide a broader understanding of the disease process of PsA.
3. In addition, this in-vivo imaging study provides the systemic burden of enthesitis (rSUVmax) in PsA. TB-PET/CT imaging will be able to quantify and monitor enthesial inflammatory burden in a patient and its therapeutic response.
A. Demonstrates in PsA inflammation of the flexor and extensor tendon of the fingers and the association of the extensor tendon with its enthesitis of the DIP joint and adjacent nail matrix inflammation. Nail matrix is inflamed sparing the nail bed along with the adjacent inflammation of the extensor tendon at the site of insertion (enthesitis)
B. Compared to PsA there is no significant enthesitis at the DIP joint in rheumatoid arthritis or in osteoarthritis.
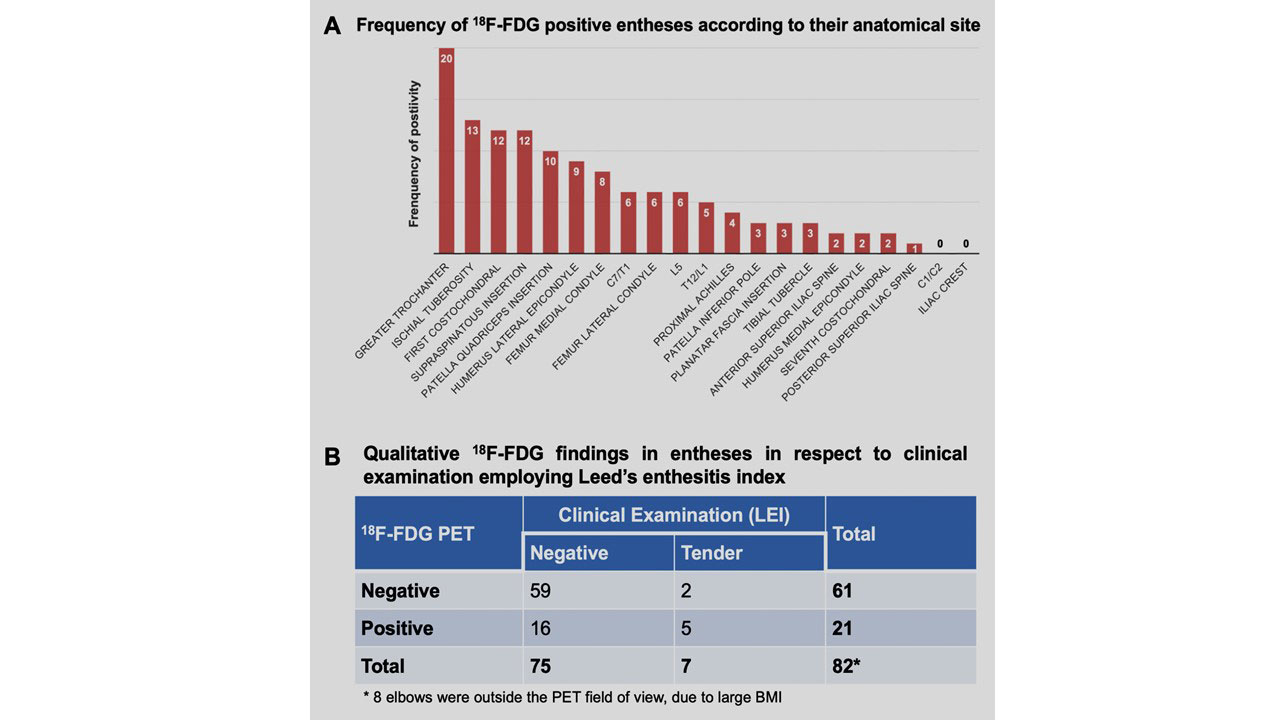
A. Frequency of positive entheses on 18F-FDG total-body PET/CT according to their anatomical site.
Fig 2. B. Association of 18F-FDG total-body PET/CT findings with the rheumatological examination in a subset of the evaluated entheses (B).
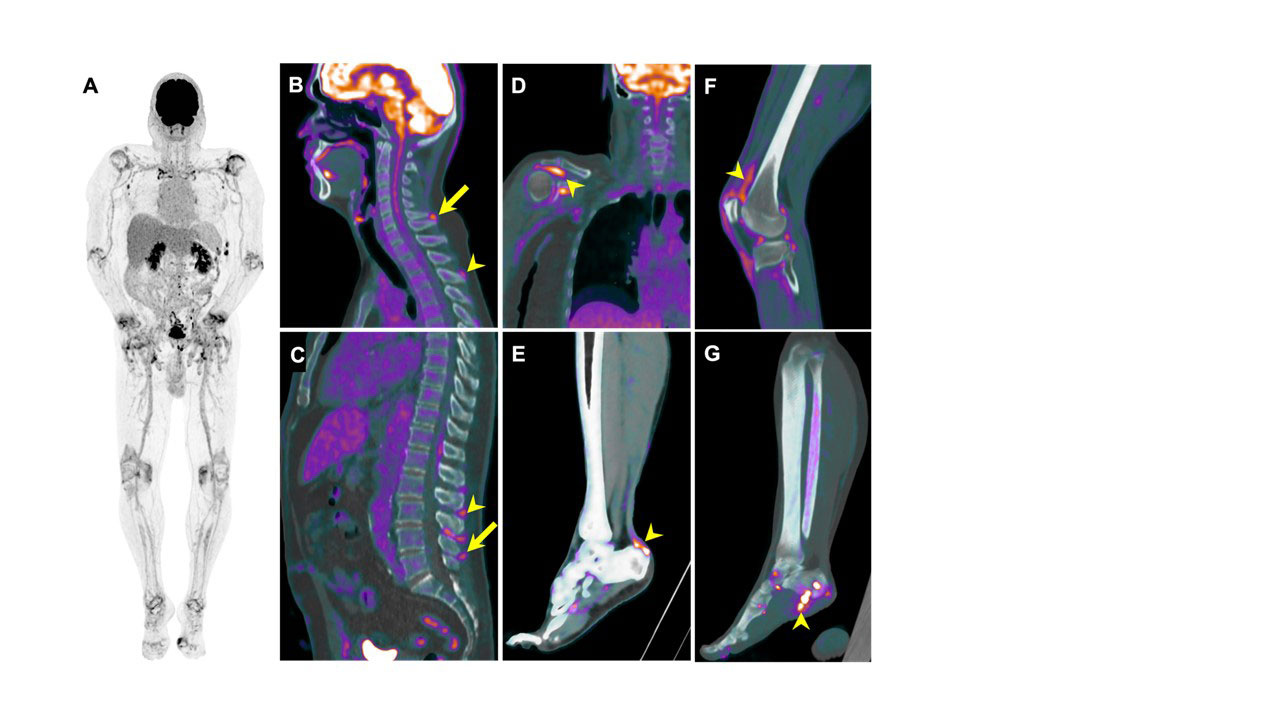
Total-Body PET/CT Evaluation of PsA: (A) Maximum-intensity projection (MIP) of a Total-Body PET scan demonstrating multiple active joints (shoulders, sternoclavicular joints, elbows, wrists, knees, ankles, left first MTP). Fused PET/CT images from different participants demonstrating enthesitis patterns throughout the body (B-G). The spine entheses are involved at the cervical (B, arrow at C7 and arrowhead at T3), and lumbar regions (C, arrow at L5 and arrowhead at L3/L4/L5 inter/supra-spinous ligaments). Other inflamed entheses include right supraspinatus (D), Achilles (E), and patellar tendons (F), and plantar fascia (G).
To cite this abstract in AMA style:
Raychaudhuri S, Abdelhafez Y, Mazza D, Raychaudhuri S, Chaudhari A. Enthesitis a Dominant Pathology in Psoriatic Arthritis: Identification and Quantification of Enthesitis Burden by 18F-FDG Total-Body PET/CT Imaging [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/enthesitis-a-dominant-pathology-in-psoriatic-arthritis-identification-and-quantification-of-enthesitis-burden-by-18f-fdg-total-body-pet-ct-imaging/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/enthesitis-a-dominant-pathology-in-psoriatic-arthritis-identification-and-quantification-of-enthesitis-burden-by-18f-fdg-total-body-pet-ct-imaging/