Session Information
Date: Saturday, November 16, 2024
Title: Metabolic & Crystal Arthropathies – Basic & Clinical Science Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Despite its prevalence, calcium pyrophosphate deposition disease (CPPD) remains insufficiently studied. Leveraging electronic health record (EHR) data, a rich source of patient information, could facilitate the automatic enrollment of CPPD patients in registries without the need for manual recruitment1, enhancing research opportunities. However, registry reliability is often compromised due to the poor accuracy of diagnostic coding for CPPD. We describe the process and validation of creating a CPPD-registry out of EHR-data from a tertiary university hospital in Geneva, Switzerland integrating various sources of information to improve its accuracy.
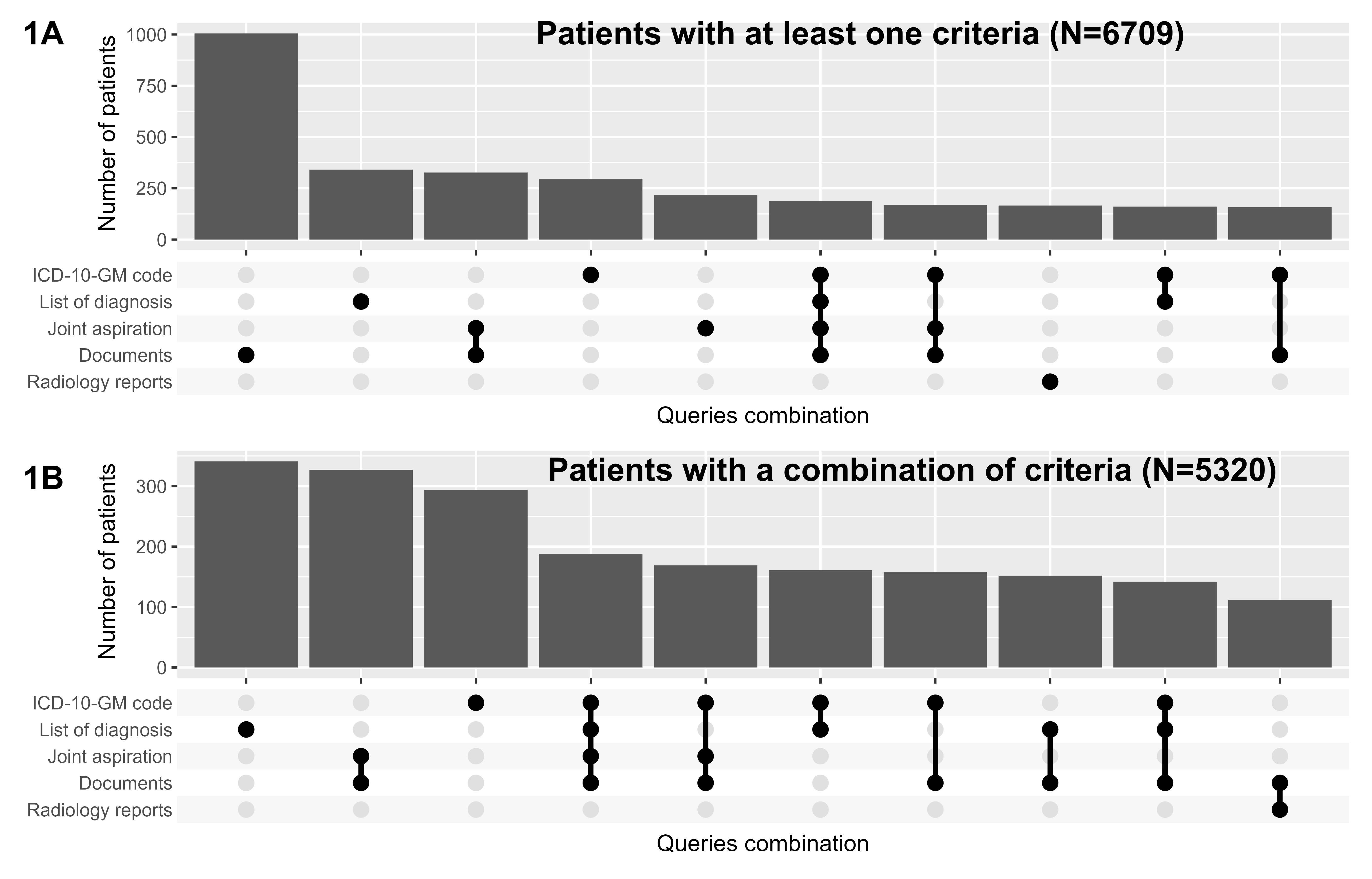
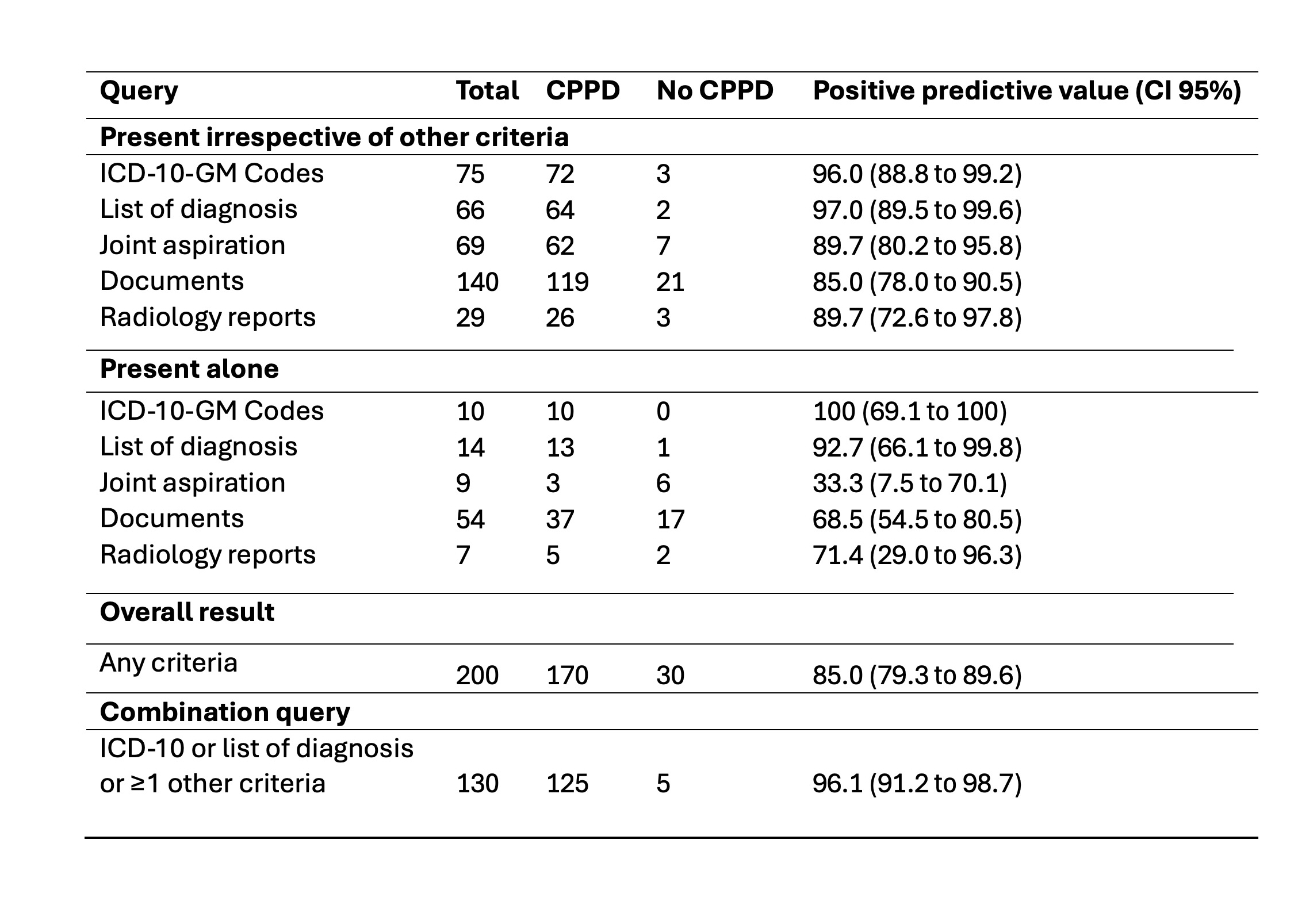
Methods: We screened EHR-data from patients over 18 years old with any out- or inpatient visit at the Geneva University Hospital—Switzerland’s largest tertiary hospital—between January 1, 2013, and December 31, 2023. Screening criteria consisted of the presence of at least one of the following: ICD-10-GM codes for CPPD (M11) OR positive joint aspiration for CPP crystal OR CPPD-related terms (“pseudogout”, “chondrocalcinosis”) in the list of diagnosis OR documents OR imaging reports. A random sample of 200 medical charts were fully reviewed by a trained nurse or physician. The positive predictive value (PPV) to detect CPPD was established if any form of it was mentioned by any doctor in any part of the EHR.
Results: The four criteria identified 6709 patients presumably suffering from CPPD (figure 1A). Most patients were identified by screening medical reports (15.0%), followed by the list of diagnosis (5.1%). 3% of the patients had a positive joint aspiration for CPPD, without any documented diagnosis in the EHR. In the randomly selected 200 charts manually reviewed (table 1), the overall (any criterion) positive predictive value was 85.0% (CI 95% 79.3 to 89.6%). When taken alone (i.e. without any other criteria), both the ICD-10 codes and the list of diagnosis showed the best PPV (respectively 100% and 92.7%). The sole use of these two criteria would decrease the number of included patients to 1953. By using a combination of criteria (ICD-10 codes OR list of diagnosis OR ≥ 1 other criteria), the PPV reached 96.1% (CI 91.2% to 98.7%), leading to a registry of 5320 patients (Figure 1B).
Conclusion: The creation of a CPPD-register with automatic enrollment is feasible and valid. Incorporating various elements of the EHR, beyond only diagnostic codes, improves patient detection accuracy and increases registry numbers. Notably, a subset of patients exhibited positive joint aspirations without a corresponding documented diagnosis, indicating a documentation gap. The next step is to estimate the negative predictive value in a sample of patients without any criteria, yet with risk factors for CPPD, and develop a method to classify CPPD patients by clinical presentation. The final register will help assess pertinent clinical outcomes using clinical indicator to evaluate current quality of CPPD care and trajectories within the disease.
To cite this abstract in AMA style:
Bürgisser N, Mongin D, Mehouachi S, Courvoisier D, Lauper K. Electronic Health Record-Based Calcium Pyrophosphate Deposition Disease Registry: A Feasibility Study [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/electronic-health-record-based-calcium-pyrophosphate-deposition-disease-registry-a-feasibility-study/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/electronic-health-record-based-calcium-pyrophosphate-deposition-disease-registry-a-feasibility-study/