Session Information
Session Type: Abstract Session
Session Time: 2:00PM-3:30PM
Background/Purpose: Knee osteoarthritis (OA) is a leading global cause of pain and disability, with no current cure. Knee pain is the most common symptom and a driving factor for patients to seek treatment for knee OA. Exercise and Corticosteroid (CS) injections are mainstays of treatment for knee OA, however, increased utilization of CS injections may increase the risk of radiographic knee OA progression and cartilage loss. Given this, physical activity (PA) may be an ideal first-line treatment, however, it is unknown if PA modifies the utilization of CS in those with varying levels of pain. Therefore, the purpose of this study was to determine if PA modifies the relationship between knee pain and utilization of CS injections during a 5-year follow-up period in adults with or at high risk for knee OA.
Methods: We used data from the Osteoarthritis Initiative (OAI). Our exposure was visual analogue scale (VAS) knee pain severity over the past 30 days, dichotomized using a patient acceptable symptom state (PASS) value into high (≥ 4) vs low pain (< 4) at the 48-month visit (analytic baseline, BL). Our outcome was receiving a CS injection. Participants were asked, “In the past 6 months, have you received a CS injection?” at the 48-, 60-, 72-, 84-, 96-, and 108-month follow-up visits. PA at BL was measured using an Actigraph GT1M and was examined as an effect measure modifier between pain and CS injection. We used 6000 steps/day to stratify the sample, as this cutoff was previously found to be associated with developing functional limitation. We excluded participants who answered yes to the CS injection question at BL. We produced Kaplan-Meier survival curves for cumulative incidence of not receiving a CS injection and used Cox proportional hazards regression to calculate discrete-time hazard ratios (HR) and 95% confidence intervals (CI), adjusted for potential confounders.
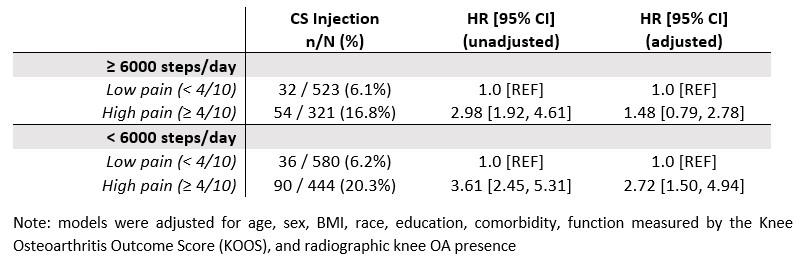
Results: 1868 participants (mean age = 65.0 years old, 55% female, mean BMI = 28.5 kg/m2) were included in the overall analytic sample. 212 participants received at least one CS injection over 5 years of follow-up. In the ≥ 6000 steps/day group, survival probability was 82.9% for those with high pain and 93.7% for those with low pain (Figure 1). In the < 6000 steps/day group, survival probability was 78.5% for those with high pain and 93.4% for those with low pain (Figure 2). Participants with ≥ 4/10 pain that walked < 6000 steps/day had a 2.72 times greater hazard of receiving a CS injection compared to those with < 4/10 pain (adjusted HR [95% CI] = 2.72 [1.50, 4.94]). Participants with ≥ 4/10 pain that walked ≥ 6000 steps/day had a 1.48 times greater hazard of receiving a CS injection compared to those with < 4/10 pain, which did not reach statistical significance (adjusted HR [95% CI] = 1.48 [0.79, 2.78]) (Table 1).
Conclusion: In adults with knee OA who walk less than 6000 steps per day, high pain is associated with greater corticosteroid utilization. However, in those who walk at least 6000 steps per day, pain is not related to CS injection utilization over the next 5 years. This initial look suggests that daily walking may modify the relationship between pain and receiving a CS injection, though further research is warranted.


To cite this abstract in AMA style:
Liles S, White D, Bye T, Jakiela J. Does Physical Activity Modify the Relationship Between Pain and Corticosteroid Injection Utilization in Adults with or at High Risk for Knee Osteoarthritis? [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/does-physical-activity-modify-the-relationship-between-pain-and-corticosteroid-injection-utilization-in-adults-with-or-at-high-risk-for-knee-osteoarthritis/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/does-physical-activity-modify-the-relationship-between-pain-and-corticosteroid-injection-utilization-in-adults-with-or-at-high-risk-for-knee-osteoarthritis/