Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Patients with RA display different trajectories in the improvement of disease activity. Discerning the RA trajectories, how they differ between patients and which factors influence them, is relevant to identify opportunities to improve disease management. To capture the full granularity we used a pseudo-time analysis on data from individual visits. We aimed to identify novel subgroups in the disease trajectories of RA patients after first visit to the rheumatology clinic.
Methods: We collected visits of early RA patients over 1.5 years from the LUMC outpatient clinic between 2011-2022 who had at least two visits (n=1,237 patients, 5,017 visits). All visits captured swollen and tender joint counts (SJC, TJC), haemoglobin, thrombocytes, MCV, leukocytes, and ESR. Time of visit, serology, sex, and age were not used for clustering. After normalisation, we clustered visits using cosine similarity and the Leiden algorithm and identified similar patient trajectories with sequence analysis methods. We validated our findings in the TACERA cohort consisting of 244 patients with early seropositive RA recruited in 2014 with a total of 750 visits with intervals of at least 6 months.
Results: The Leiden data showed eight disease states (DSs) with SJC/TJC, ESR and leukocytes as the major discriminating factors (Fig 1A & C). DS1 was the clinically optimal DS with the least inflammation overall. Though each cluster contained visits from baseline until the last visit (within 1.5 years), the low disease activity DSs were on average enriched for later visits (Fig 1B & D). The disease state sequences consisted of 4 distinct trajectories (Fig 1E) that were characterised by either blood or joint inflammation:
A – high ESR clusters at start and end, ending in suboptimal DS2 (DS6 >DS5 >DS2);
B – starting with high SJC/TJC and rapid progression towards the ideal DS1;
C – transition and/or ending in high leukocyte DS3;
D – high SJC/TJC, poor prognosis, not reaching low SJC/TJC (DS4 >DS7).
In the independent analysis on TACERA, we found similar DS and trajectories. The only differences between the two were an intermediate SJC/TJS Tacera-DS-9 (Fig 1A & C) and the very early Leiden-DS-8.
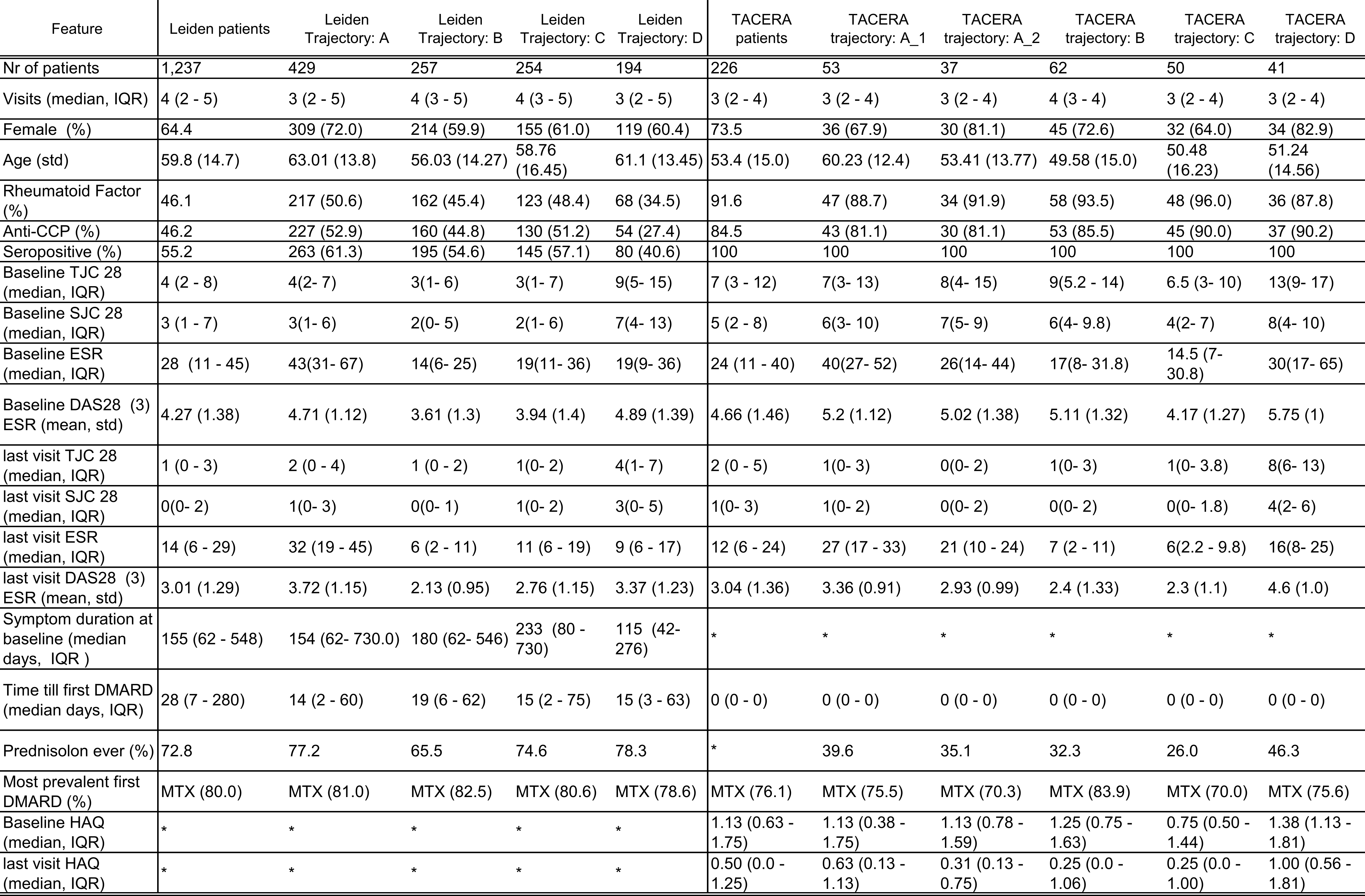
The trajectories and DSs differed in age, sex, and serostatus, even though these variables were not included in the clustering (Table 1). The trajectories were not driven by inclusion date, follow-up duration, symptom duration or time till methotrexate initiation. Patients in trajectories A and C ended with almost similar SJC & TJC as those in trajectory-B but still had increased blood inflammation. There is a discrepancy between the trajectories and levels of patient-reported outcomes (PROs) experienced over time: B has a steady decline in all PROs, A is stable on average after 6 months, and C has a great early trajectory but deteriorates again after one year.(Fig 2).
Conclusion: With our pseudo-time analysis we identified and replicated 4 trajectories in early RA. These trajectories draw a granular picture of different patients stranding in suboptimal disease states, particularly if their disease was marked by inflammation in blood instead of the joints These results provide insights into opportunities for improving care and possible differentiation of disease aetiology.
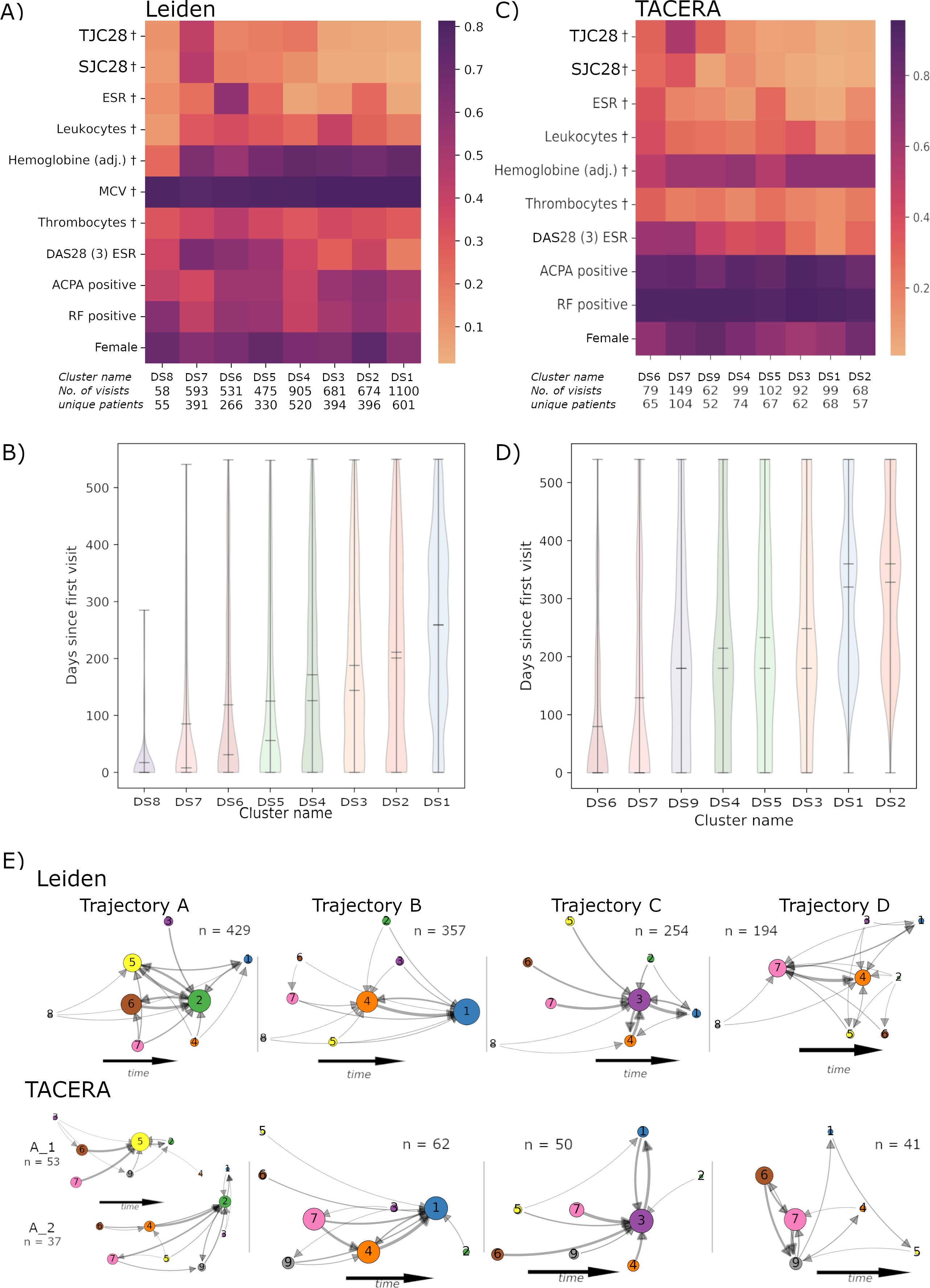
Clusters are coloured consistently between B, D & E.
† = variables used for clustering, DS = disease state.
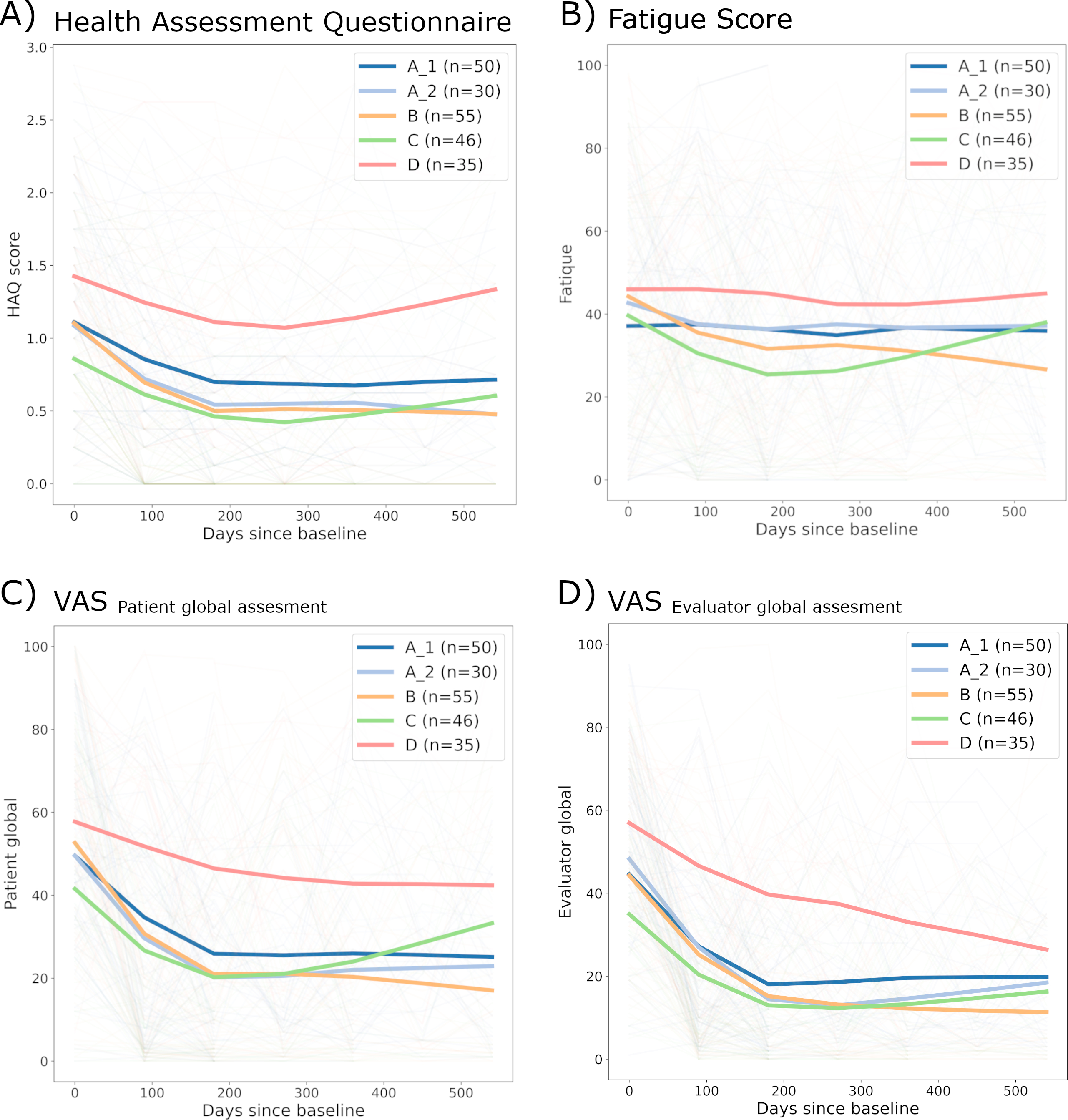
A) depicts the trend of HAQ score.
B) depicts the amount of fatigue reported by patients.
C) depicts the amount of disease activity experienced by patients.
D) depicts the amount of disease activity assessed by the rheumatologist.
To cite this abstract in AMA style:
Steinz N, Maarseveen T, Cope A, Isaacs J, Winkler A, Huizinga T, Abraham Y, Knevel R. Dissecting Early RA Patient Trajectories Through Time-independent Disease State Identification Identifies Distinct Patterns Dissected by Inflammation in Blood or Joints [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/dissecting-early-ra-patient-trajectories-through-time-independent-disease-state-identification-identifies-distinct-patterns-dissected-by-inflammation-in-blood-or-joints/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/dissecting-early-ra-patient-trajectories-through-time-independent-disease-state-identification-identifies-distinct-patterns-dissected-by-inflammation-in-blood-or-joints/