Session Information
Session Type: Poster Session A
Session Time: 8:30AM-10:30AM
Background/Purpose: Cognitive flexibility, a process that enables goal-oriented cognitive switching between mental function modes, is central to executive function which is impaired in SLE patients. Multimodal integration of brain network anatomy and functional signals has recently been shown to mediate the cognitive switching process. Specifically, alignment between blood-oxygenation-level-dependent (BOLD) signals and the architecture of the underlying white matter (WM) network is associated with higher cognitive flexibility. In SLE patients, whether WM networks that constrain brain dynamics during cognitive switching is altered remains unknown. Here, brain structural-functional alignment and liberality between SLE patients and healthy controls (HC) were studied by performing the Modified Wisconsin Card Sorting Test (MCST) that probed cognitive flexibility. We hypothesized that the structural-functional integration of the executive control network (ECN) would be disrupted, with behavioral implications in SLE patients.
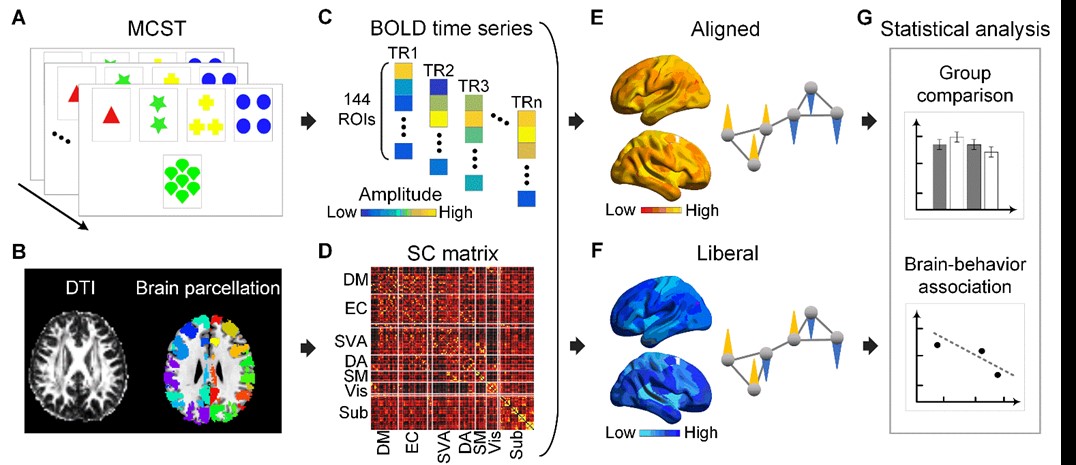
Methods: We studied 17 SLE patients without neuropsychiatric manifestation (aged 33.3±7.9 years) and 44 HC (aged 28.3±8.2 years). Functional brain magnetic resonance imaging (MRI) during MCST, T1-weighted structural and diffusion MRI were conducted. Region-of-interest (ROI) time series were extracted using a 144-ROI brain functional parcellation scheme. We constructed the anatomical brain network by defining the connectivity between each pair of ROIs as the normalized connection probability derived from probabilistic diffusion tractography. BOLD signals were decomposed into a proportion that aligned with the anatomical network and a proportion that indicated liberality (Fig. 1). We performed group comparison on alignment and liberality at the global and network levels using two-sample t-tests (a=0.05) and evaluated their relationships with MCST performance.
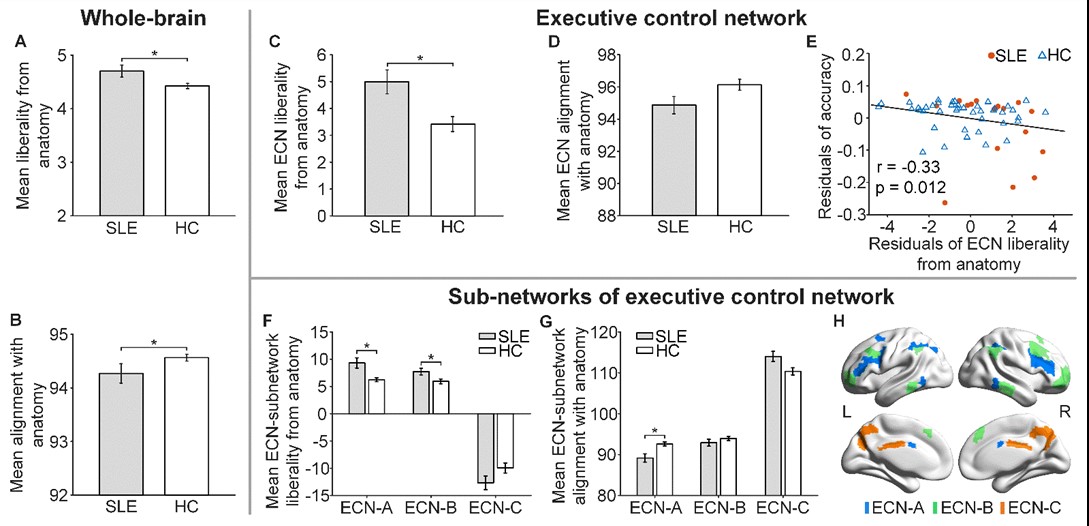
Results: The two groups did not differ in overall MCST performance. SLE patients showed higher global functional liberality and lower global functional alignment with the structural networks during MCST (p=0.014 and 0.045, respectively) compared to HC. At the network level, SLE patients showed higher liberality in the ECN compared to HC (FDR-corrected, p=0.026). Focusing on the 3 ECN sub-networks (Fig. 2H), the abnormality of functional organization atop the ECN anatomy was driven by the lower alignment in ECN-A and higher liberality in ECN-A and ECN-B in SLE patients (FDR-corrected p=0.007, 0.008 and 0.026, respectively). ECN-A and ECN-B are the typical lateral fronto-parietal executive control regions while ECN-C is near to the default mode network. Higher liberality and lower alignment were correlated with reduced task accuracy (p< 0.05). The correlation between ECN liberality and task accuracy remained significant (p=0.023) after controlling for global liberality and alignment.
Conclusion: Our study demonstrated reduced functional-structural alignment of the ECN in SLE patients using a novel graph signal processing method that constrained BOLD signal magnitude to the anatomical network architecture. Reduced functional-structural alignment was associated with poorer cognitive switching performance.
To cite this abstract in AMA style:
Qian X, Bassett D, Ng K, Loo B, Koh A, Zhou J, Mak A. Disrupted Executive Control Network Structural-Functional Integration Is Associated with Inferior Performance of Cognitive Switching Tasks in Patients with Systemic Lupus Erythematosus (SLE) [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/disrupted-executive-control-network-structural-functional-integration-is-associated-with-inferior-performance-of-cognitive-switching-tasks-in-patients-with-systemic-lupus-erythematosus-sle/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/disrupted-executive-control-network-structural-functional-integration-is-associated-with-inferior-performance-of-cognitive-switching-tasks-in-patients-with-systemic-lupus-erythematosus-sle/