Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: The diagnosis of serositis in systemic lupus erythematosus (SLE) relies on combining clinical and serological data, alongside imaging studies. The aim of this study was to evaluate the diagnostic performance of anti-dsDNA antibodies in pleural, ascitic and pericardial fluid for the diagnosis of lupus serositis.
Methods: This retrospective study enrolled patients aged over 18 years with pleural effusion, ascites, or pericardial effusion admitted to a tertiary center in Mexico City between 2017-2024. The study included patients who underwent assessment for anti-dsDNA antibodies in their effusion samples. Patients were classified into three groups based on their final clinical diagnoses: lupus serositis (group 1), non-SLE related effusion in lupus patients (group 2), and patients with effusion without lupus diagnosis (group 3). The diagnosis of SLE was determined according to the ACR/EULAR 2019 criteria. Demographic, clinical, and serological variables were collected. Disease activity and damage accrual were assessed using the SLEDAI-2K and the SDI. Serum levels of anti-dsDNA antibodies and complement fractions were also recorded. Anti-dsDNA IgG antibody levels in both serum and effusion were quantified using automated ELISA. The optimal cut-off point for anti-dsDNA antibodies in effusion and its ratio with serum levels were determined using the Youden index, and diagnostic statistics were calculated for each cut-off point.
Results: Thirty-one patients with effusion samples were included (15 pleural, 12 ascites and 4 pericardial effusion samples). Group 1: 16 lupus serositis, Group 2: 8 non-SLE-serositis and Group 3: 7 effusions without SLE. Age, disease duration and damage accrual between SLE groups were similar. Patients in group 1 exhibited significantly higher disease activity compared to group 2 (SLEDAI 2K 10 vs. 1, p=0.003) and more presence of lupus nephritis (68.8% vs. 0%, p=0.002). Group 1 showed lower serum complement levels (C3 36 mg/dL vs. 80 mg/dL vs. 84 mg/dL, p=0.001; C4 8 mg/dL vs. 21 mg/dL vs. 27.5 mg/dL, p< 0.001) and higher serum anti-dsDNA (203.2 IU/mL vs. 14.25 IU/mL vs. 4.0 IU/mL, p=0.013) than the other groups. Patients in group 1 had elevated effusion levels of anti-dsDNA (529.4 IU/mL vs. 1.80 IU/mL vs. 78.2 IU/mL, p=0.003) compared to the groups. The optimal cut-off points to identified lupus serositis was >118.0 IU/mL for anti-dsDNA in effusion (AUC 0.859, sensitivity 68.8%, specificity 91.7%, Youden Index 0.605) and an effusion/serum ratio of anti-dsDNA >0.4 (AUC 0.731, sensitivity 92.3%, specificity 66.7%, Youden Index 0.590) (Table 1).
Conclusion: Patients with lupus serositis showed higher disease activity. Effusion levels of anti-dsDNA >118 IU/mL demonstrated high specificity for lupus serositis, while the effusion/serum ratio of anti-dsDNA >0.4 exhibited high sensitivity for lupus serositis. Effusion levels of anti-dsDNA and the serum/effusion ratio of anti-dsDNA could be useful for diagnosing lupus serositis.
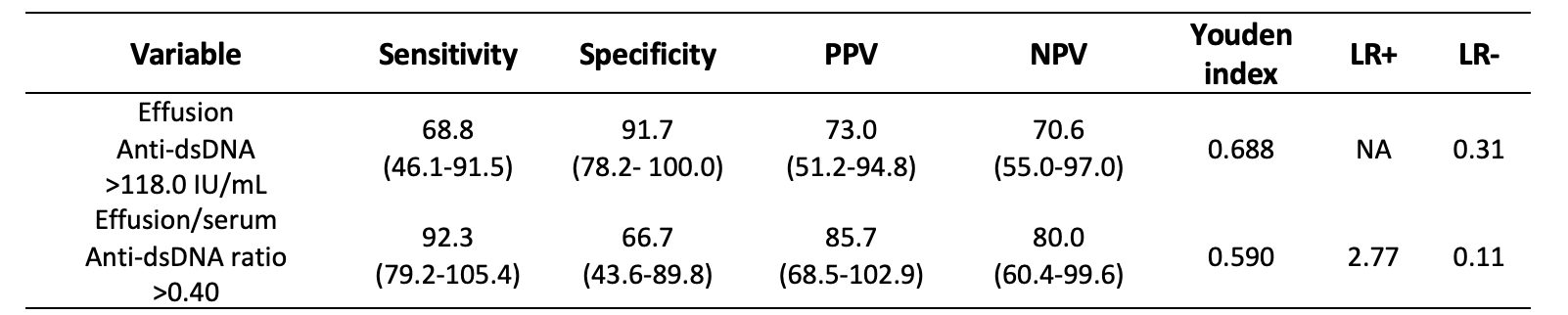
Data are expressed as percentages (95% confidence intervals). PPV: positive predictive value; NPV: negative predictive value; LR+: positive likelihood ratio, LR-: negative likelihood ratio, NA: not assessed.
To cite this abstract in AMA style:
Sandino-Bermúdez M, Cimé-Aké E, Campos-Guzmán J, Briones-García E, G. Lazarini E, Núñez-Álvarez C, Fragoso-Loyo H. Diagnostic Performance of Anti-dsDNA Antibodies in Pleural, Ascitic and Pericardial Fluid for Lupus Serositis: Experience of a Tertiary Center in Mexico [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/diagnostic-performance-of-anti-dsdna-antibodies-in-pleural-ascitic-and-pericardial-fluid-for-lupus-serositis-experience-of-a-tertiary-center-in-mexico/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/diagnostic-performance-of-anti-dsdna-antibodies-in-pleural-ascitic-and-pericardial-fluid-for-lupus-serositis-experience-of-a-tertiary-center-in-mexico/