Session Information
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Dermatomyositis (DM) can be categorized into two major subtypes: clinically amyopathic dermatomyositis (CADM) and classic dermatomyositis (CDM). In this study, we aimed to identify characteristics of the patients with DM evaluated at the combined Dermatology-Rheumatology clinic.
Methods: We used ICD-9/10 codes to identify patients with DM. Demographics, clinical features, laboratory values, type cancer diagnosis (if any) was obtained by electronic medical records. We used descriptive statistics to present characteristics of patients. The association between a variety of factors and risk of cancer was examined using logistic regression.
Results: 33 patients with DM were identified. 8 (24%) were male and 25 (76%) were female. The average age at diagnosis was 50 (SD:17). 61% had CDM, 39% had CADM. 70% White, 12% Hispanic, 6% Black, 3% Asian and 9% unknown (Figure 1). Medications used by patients for DM in order of frequency (n, %) include prednisone (21, 64 %), hydroxychloroquine (20, 61 %), methotrexate (14, 42%), azathioprine (9, 27%), intravenous immunoglobulin (6, 18%), mycophenolate mofetil (3, 9%), rituximab (3, 9%), and thalidomide (1, 3%) (Figure 2). Pulmonary disease with restrictive pattern 6 (18%), esophageal involvement 7 (21%), calcinosis cutis 4 (12%) and panniculitis were reported in 2 (6%) of the patients (Figure 3). Muscle enzymes were high in 20 (61%), normal in 9 (27%) and unknown in 4 (12%). Positive antinuclear antibodies were reported in 52%, majority with speckled pattern. One patient had juvenile DM. 36% (n=12) had a history of cancer, including breast 12%, prostate 6%, T-cell lymphoma, gastric lymphoma, non-small cell lung cancer, cervix, squamous cell carcinoma (SCC) of the tonsil and invasive skin SCC, each one 3%. Three cancer cases occurred within 1 year, 5 cases within 5 years and 4 cases more than 5 years before/after the diagnosis of DM. Average age at diagnosis for patients with cancer was 57 (SD: 12) and for patients without cancer was 45 (SD: 19) (Figure 4). We found no evidence of an association between gender, type of DM, enzyme level, pulmonary involvement, obesity, positive ANA and cancer. History of current or former smoking was strongly associated with increased risk of cancer (OR: 7.50, 95% CI: 1.49-37.66) (Figure 5).
Conclusion: Our results show a higher prevalence of cancer among DM patients compared to the general population. The average age at diagnosis of DM was higher in patients with cancer. We found no association between gender and cancer which is in contrast to previous studies that reported higher risk of malignancy in males compared to females. Smoking (ever versus never) was strongly associated with cancer. This can be explained by the synergistic effect of smoking in patients with DM. No association between pulmonary involvement and cancer was found. Limitations include small sample size and retrospective study design.
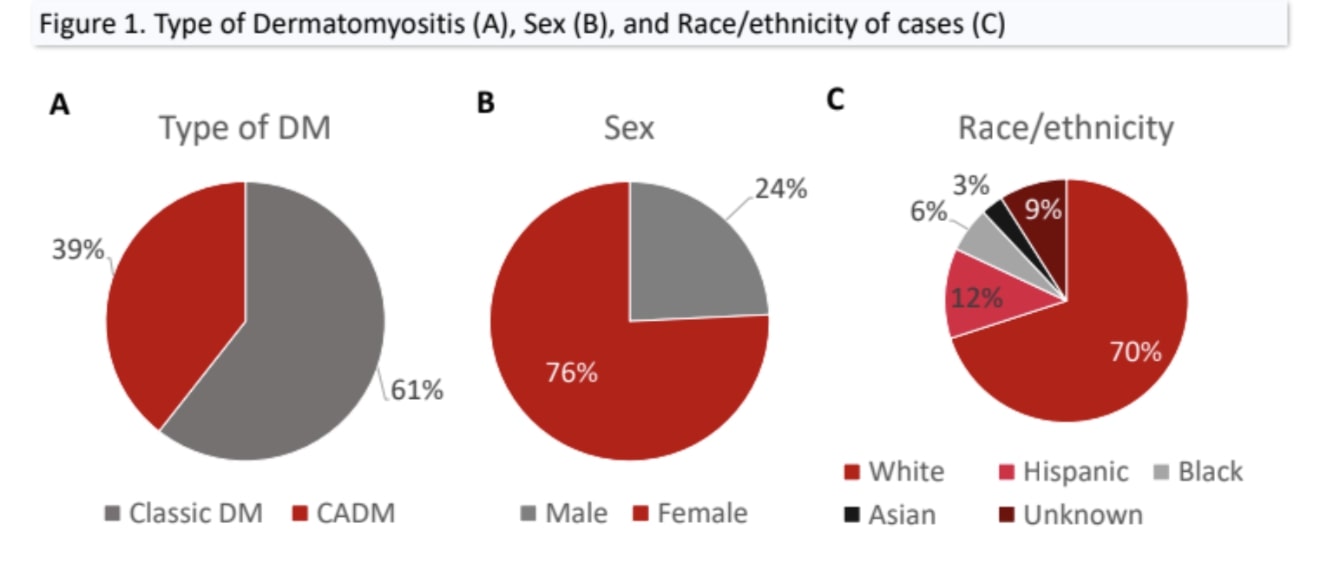 Figure 1: Type of Dermatomyositis (A), Sex (B), and Race/ethnicity of cases (C)
Figure 1: Type of Dermatomyositis (A), Sex (B), and Race/ethnicity of cases (C)
 Figure 2: Type and frequency of medications used by cases Figure 3: Prevalence of pulmonary disease, esophageal involvement, calcinosis cutis, and panniculitis
Figure 2: Type and frequency of medications used by cases Figure 3: Prevalence of pulmonary disease, esophageal involvement, calcinosis cutis, and panniculitis
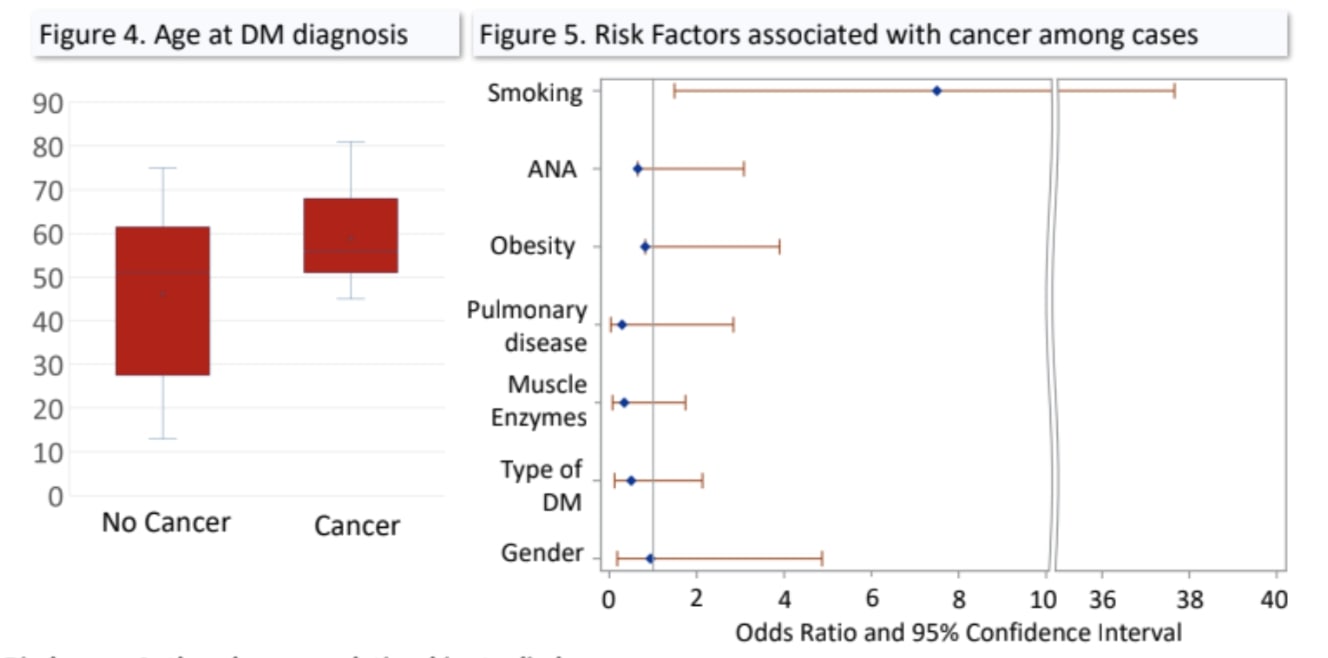 Figure 4: Age at DM diagnosis Figure 5: Risk Factors associated with cancer among cases
Figure 4: Age at DM diagnosis Figure 5: Risk Factors associated with cancer among cases
To cite this abstract in AMA style:
Elkiran B, Tajalli M, Vance T, Qureshi A, Reginato A. Dermatomyositis: A Dermatology-Rheumatology Clinic Retrospective Analysis [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/dermatomyositis-a-dermatology-rheumatology-clinic-retrospective-analysis/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/dermatomyositis-a-dermatology-rheumatology-clinic-retrospective-analysis/