Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
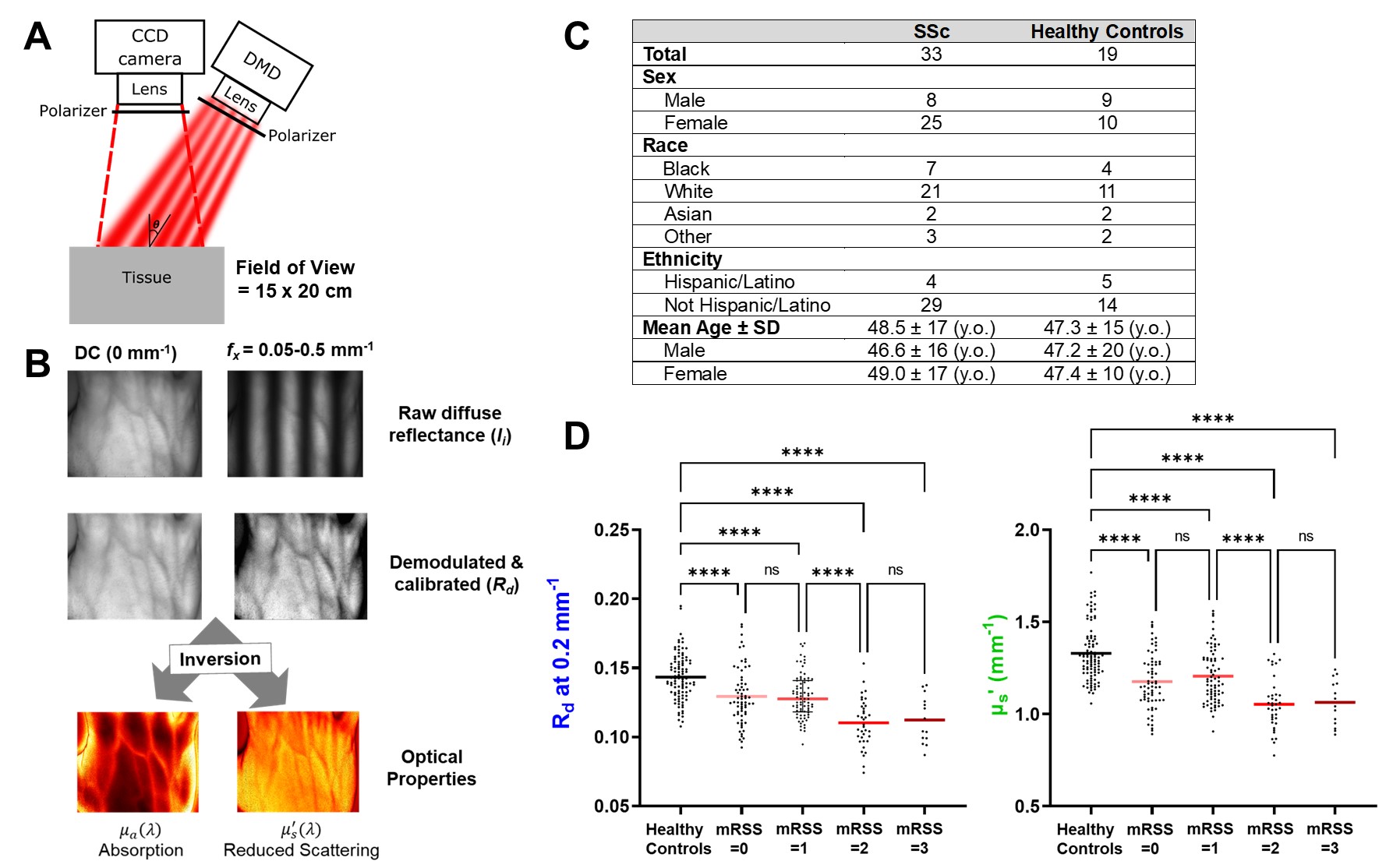
Background/Purpose: The modified Rodnan skin score (mRSS) is the gold standard for scleroderma (SSc) skin assessment, yet it suffers from subjectivity and interrater variability. Spatial Frequency Domain Imaging (SFDI) utilizes near-infrared light to quantify optical tissue properties like diffuse reflectance (Rd) and reduced scattering coefficients (μs´) (Fig. 1A). In a small pilot study, we demonstrated SFDI’s ability to detect skin changes in SSc, with excellent intra- and inter-rater reliability (1). Our present study further evaluates SFDI in a larger cohort of SSc patients and controls, as well as its ability to detect longitudinal skin changes in SSc. The correlation of SFDI with local durometry, ultrasound thickness and histology scores were also assessed.
Methods: 33 SSc patients with early diffuse SSc (< 5 years) and 19 healthy controls were enrolled. SFDI parameters (μs´ and Rd measured at 0.2 mm-1 and 851 nm) were recorded from 6 sites: left/right forearms, hands, and fingers. Dermal thickness was measured using high frequency ultrasound (HUS) with a 20 MHz probe at the mid-dorsal forearm, and a skin biopsy was collected at the same location. The mRSS was measured using the averaging method by a trained physician blinded to SFDI and HUS measurements. H&E skin sections were assessed for overall collagen fiber thickening using a 0-3 visual scoring system, and alpha smooth muscle actin (ASMA) positive fibroblast score was assessed on a VAS after exclusion of adnexal structures and vasculature. Longitudinal data was available for 10 SSc patients, and change in SFDI scores were compared to change in mRSS and HUS scores in each patient. Spearman correlation (rs) was used to calculate correlation coefficients.
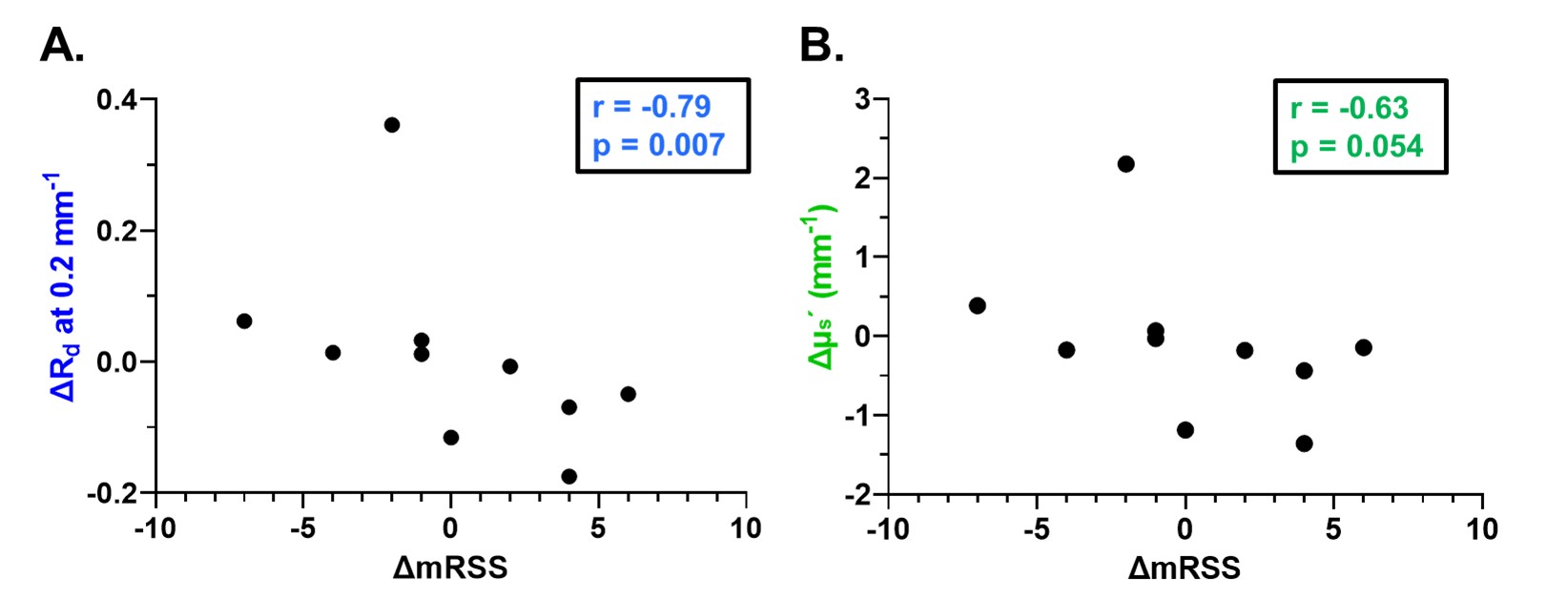
Results: In single time point analyses, healthy controls exhibited significantly higher μs´ and Rd values than SSc subjects, even in patients with no evident skin thickening by mRSS (mRSS=0), suggesting that SFDI can reveal subclinical skin changes in SSc (Fig 1D). At the biopsy site, both SFDI parameters showed significant correlations with the collagen fiber thickness scores (H&E) and fibroblast activation scores (ASMA). Forearm SFDI parameters had a significant correlation with local mRSS, local hardness (durometry score) and local dermal thickness (HUS score), as shown in Table 1. Analysis of longitudinal changes in SFDI parameters revealed a strong correlation between changes in Rd (∆Rd) and changes in mRSS (∆mRSS) (rs = -0.79, p = 0.007, Fig 2A) and good, albeit not significant, correlations between ∆μs´ and ∆mRSS (rs = -0.63, p = 0.054 Fig 2B), likely due to the small sample size. Similar results were obtained when comparing changes in SFDI with changes in HUS (rs=0.65, p=0.06 for ∆Rd and rs=0.6, p=0.09 for ∆μs´).
Conclusion: SFDI can distinguish early skin changes in systemic sclerosis (SSc) from healthy controls and provides a comprehensive view of SSc-related alterations, including dermal thickness, skin hardness, and collagen content. Furthermore, SFDI shows promise in tracking longitudinal skin changes in SSc patients, making it a versatile tool for monitoring disease progression and treatment response.
References:
Pilvar A, et al. Biomed Opt Express. 2023;14(6):2955. doi:10.1364/BOE.489609

To cite this abstract in AMA style:
Vo H, Mehendale A, Chaudhari M, El adili F, Browning J, York M, Trojanowski M, Kissin E, Roblyer D, Bujor A. Comprehensive Skin Assessment in Systemic Sclerosis Using Spatial Frequency Domain Imaging (SFDI) [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/comprehensive-skin-assessment-in-systemic-sclerosis-using-spatial-frequency-domain-imaging-sfdi/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/comprehensive-skin-assessment-in-systemic-sclerosis-using-spatial-frequency-domain-imaging-sfdi/