Session Information
Session Type: Poster Session D
Session Time: 8:30AM-10:30AM
Background/Purpose: Multimorbidity is common in patients with rheumatoid arthritis (RA), and it is associated with poor outcomes. The literature on multimorbidity suffers from numerous definitions that make comparisons difficult. We aimed to use our population-based cohort to validate a list of morbidities proposed by England et al. (ARD 2020).
Methods: In this retrospective, population-based study, residents of a geographically well-defined area with prevalent RA on 1-1-2015 were identified from a comprehensive medical record linkage system. Age and sex-matched non-RA comparators were selected from the same underlying population. Diagnostic codes were retrieved for a 5-year period prior to the prevalence date. Using 2 codes at least 30 days apart, the 44 morbidities described by England were defined, as well as 78 Clinical Classification Software (CCS) categories with chronic disease flags that did not overlap with the 44 morbidities. Rheumatoid arthritis and categories likely representing diagnostic uncertainty with RA (e.g., lupus, polymyalgia rheumatica) were excluded from the morbidities for comparability between cohorts. False discovery rate methods were used to compare the prevalence of each morbidity in the RA vs non-RA cohorts adjusting for multiple comparisons.
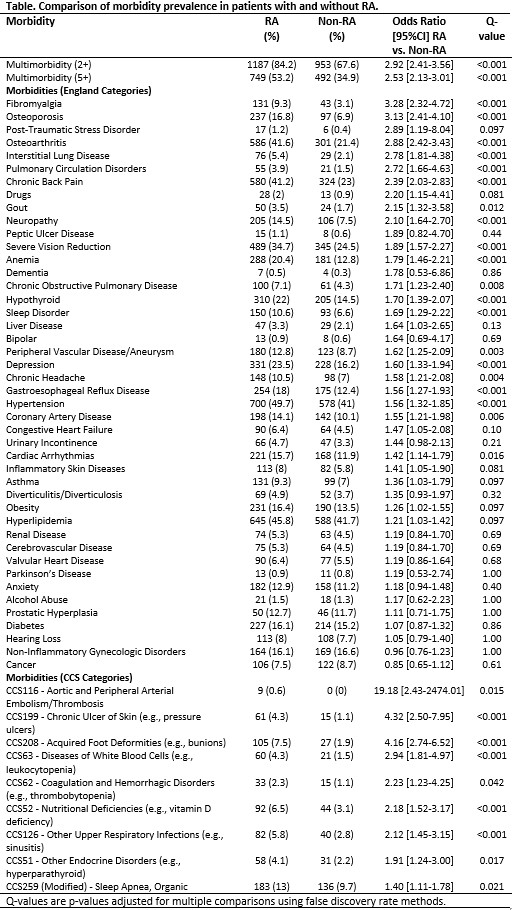
Results: A total of 1409 patients with prevalent RA (72% female; 92% Caucasian; mean age 63.5 years) and 1409 non-RA (72% female; 90% Caucasian; mean age 63.4 years) were studied with 96% of RA and 90% of non-RA having at least 5 years of prior medical history. Multimorbidity (defined as 2+ morbidities) was present in 1187 (84%) of RA and 953 (68%) of non-RA subjects using the 44 morbidities with 5+ morbidities present in 749 (53%) of RA and 492 (35%) of non-RA (p< .001 for both). RA patients had significantly higher prevalence compared to non-RA of 20 of the 44 morbidities with 33 of 44 morbidities yielding OR >1.20 (Table). The modest sample size of this cohort may have reduced the number of significant findings compared to the original report on the 44 morbidities. Among the additional 78 CCS categories, 9 were significantly higher in RA than non-RA. The majority of these morbidities (i.e., embolism/thrombosis, organic sleep disorders, hyperparathyroidism, vitamin D deficiency, chronic skin ulcers, and foot deformities) are known to be more common in patients with RA. Some morbidities (i.e., thrombocytopenia, leukopenia, other upper respiratory infections) could reflect complications of RA therapy.
Conclusion: Patients with RA have a higher prevalence of multimorbidity compared to non-RA subjects. These results validate the previously published list of 44 morbidities, and only identify a small number of other morbidities to consider in patients with RA. Further research is needed to unify the list of morbidities used to study multimorbidity in patients with RA.
To cite this abstract in AMA style:
Crowson C, Gunderson T, Myasoedova E, Atkinson E, Kronzer V, Coffey C, Davis J. Comprehensive Assessment of Multimorbidity Burden in a Population-based Cohort of Patients with Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/comprehensive-assessment-of-multimorbidity-burden-in-a-population-based-cohort-of-patients-with-rheumatoid-arthritis/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/comprehensive-assessment-of-multimorbidity-burden-in-a-population-based-cohort-of-patients-with-rheumatoid-arthritis/