Session Information
Date: Tuesday, November 14, 2023
Title: (1895–1912) Measures & Measurement of Healthcare Quality Poster II
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Patients with Rheumatoid Arthritis (RA) are at increased risk of cardiovascular disease (CVD). Despite multiple CVD risk tools available, reliability to RA population is limited as they might not fully incorporate the unique risk factors faced by this population cohort. Studies have shown a direct correlation between RA disease severity and increased prevalence of CVD risk factors like diabetes and arthrosclerosis. [1,2] Based on these findings, we can expect an adequate tool designed to assess the burden of cardiovascular disease risk should reflect the disease severity in patients with RA. We aim to assess the reliability of current CVD assessment tools used in patients with RA by comparing the strength of correlation between these tools with the RA disease severity.
Methods: A single centered retrospective observational analysis was conducted. Medical records of 102 patients all of whom met 2010 ACR/EULAR criteria were included including the DAS-28 score calculated per rheumatologist. SPSS was utilized to assess the strength and direction of the relationship between each CVD assessment tool and RA disease activity. For the former, we employed ASCVD, Framingham and mSCORE. The mSCORE risk assessment tool was recommended by EULAR to access CVD risk in patients with RA. [1] Correlational analysis between CVD assessment tools and DAS-28 score was performed to evaluate the relationship between CVD risk and disease activity. Statin use in patients at risk as recommended by the AHA were reviewed.
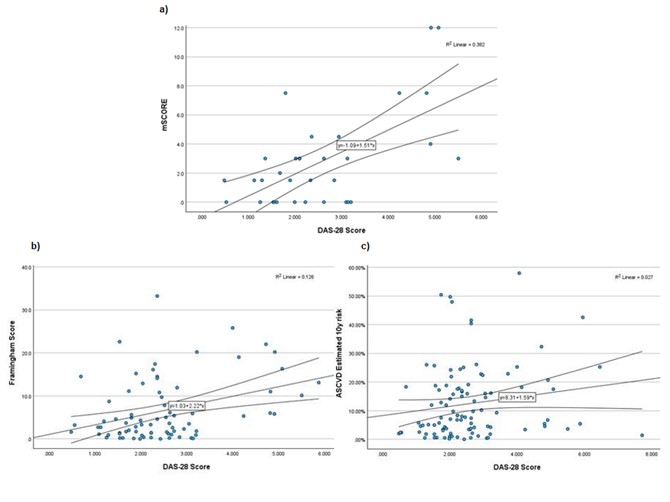
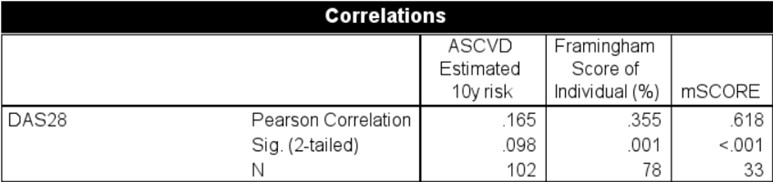
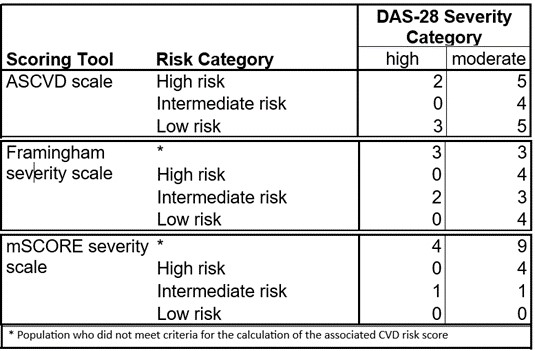
Results: Results revealed the correlational coefficient for mSCORE, Framingham score and ASCVD score with DAS-28 score where 0.618, 0.355, 0.165 with P value of < 0.001, 0.001 and 0.098 respectively (Table 1). These findings suggest that mSCORE shows the strongest correlation with DAS-28 scores compared to ASCVD and Framingham score (Figure 1). Further, we identified the number of patients with moderate to high disease activity that are calculated to have a low CVD risk. Increased variability among the tools raises questions about the accuracy of these tools in reflecting the true risk. We found that 42% (n=8) patients and 21% (n=4) who had moderate to high risk were classified as low risk in ASCVD and Framingham score respectively. At the same time, for the mSCORE, none of the patients with moderate to high disease activity was classified as low risk(Table 2). These findings reinforce our previous result.
Conclusion: Being explicitly designed for RA patients, mSCORE is likely to capture the cardiovascular risk profile of these individuals better as it incorporates RA-specific factors. Although such RA-specific tools offer some improvement over general population-based tools, their practical application remains challenging due to several experimental limitations. As a result, providers often rely on general tools leaving a concern that these patients are not being appropriately treated. Moreover, we are observing treatment failures even with currently used general risk assessment tools. Approximately 32% (n=20) in our study, who warranted statin therapy based on their ASCVD risk were not receiving it. These findings draw attention to a significant gap in adequate management of cardiovascular health in this population.
To cite this abstract in AMA style:
Shrestha P, Larsen P, Weilg Espejo P. Comparative Analysis of Existing Tools in Assessing Cardiovascular Risk in Patients with Rheumatoid Arthritis: Exploring the Inadequacies [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/comparative-analysis-of-existing-tools-in-assessing-cardiovascular-risk-in-patients-with-rheumatoid-arthritis-exploring-the-inadequacies/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/comparative-analysis-of-existing-tools-in-assessing-cardiovascular-risk-in-patients-with-rheumatoid-arthritis-exploring-the-inadequacies/