Session Information
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Patient-reported outcomes (PROs) measure a patient’s health-related quality of life. The role of ESSPRI and PROMIS measures in identifying subsets of patients with Sjogren’s disease is not established and longitudinal stability of these measures has not been assessed. This study uses PRO-based clustering to define distinct patient populations and measure cluster attribution in individual patients over time.
Methods: Data from 467 patients meeting ACR2016 criteria for Sjogren’s disease with at least 1 complete set of PRO data (ESSPRI Dryness/Fatigue and Pain and PROMIS Physical function/Ability to participate/Sleep Interference/Anxiety and Depression) were extracted from the Epic Electronic Health Record system. Baseline Clustering was completed using k-means clustering algorithm. For longitudinal analysis, an alluvial plot of 198 patients with at least two visits with complete PRO data was created to visualize transitions of patients between clusters. Statistical analysis between clusters was done using ANOVA, Chi-squared, and Fisher’s exact tests.
Results: K-means algorithm identified 4 clusters of patients at baseline: cluster 1 (77/467; 16.5%), Low symptoms/high function (LSHF), cluster 2 (130/467; 27.8%), High symptoms/balanced function (HSBF), cluster 3 (116/467; 24.8%), Moderate symptoms/balanced function (MSBF), and cluster 4 (144/467; 30.8%), High symptoms/poor function (HSPF) (Figure 1). Demographic variables, including age, sex, and race, anti-SSA/Ro positivity, disease phenotypic markers and DMARD exposure did not differ between clusters (Table 1). Abnormal salivary flow was least frequent in the LSHF cluster (29/77; p=0.008 by Chi-squared test). Abnormal Schirmer’s and hypergammaglobulinemia were least frequent in the HSPF cluster (95/144;70.4% p=0.012 and 40/144; 28.6% p=0.025 by Chi-squared test, respectively). Longitudinal analysis of cluster stability in 198 patients over 2 to 4 visits demonstrated that most patients (54.0%) remained in the same cluster over time (Figure 2). Transitions between extreme clusters (LSHF and HSBF) were significantly less frequent than other transitions (3/35 vs 93/96; p< 1X1022, Fisher’s exact test).
Conclusion: ESSPRI and PROMIS measures define distinct clusters in patients with Sjogren’s disease. Cluster attribution of individual patients remains relatively stable over time and changes between extreme clusters is rare. Prospective studies are needed to further define the relationship between cluster stability, disease flares and response to therapy.
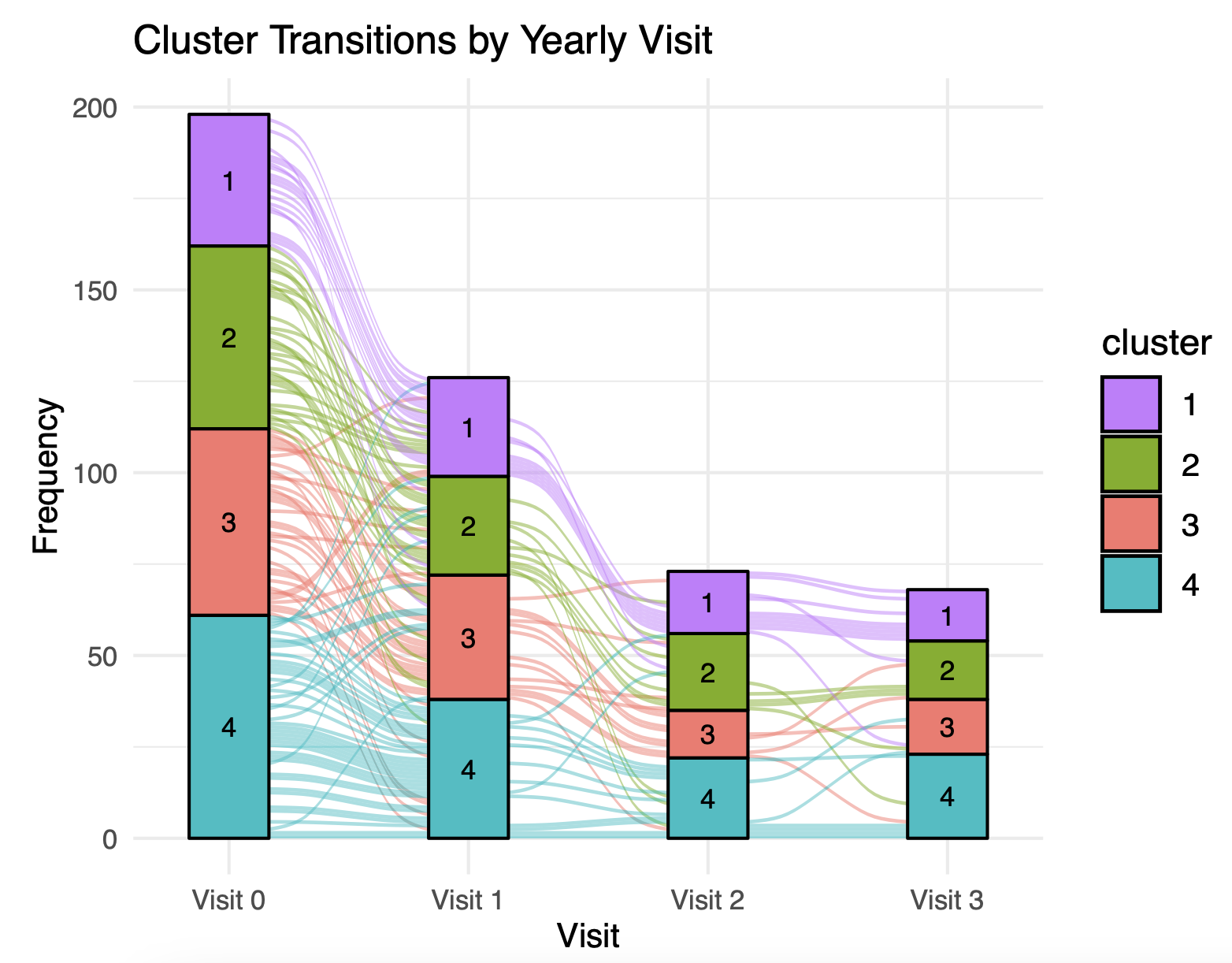 Table 1: Baseline characteristics in clusters of patients with Sjogren’s disease. 1 Adjusted n to account for missing data. 2 Ever present. Abbreviations: LSHF (low symptoms/high function), HSBF (high symptoms/balanced function), MSBF (moderate symptoms, balanced function), HSPF (high symptoms/poor function
Table 1: Baseline characteristics in clusters of patients with Sjogren’s disease. 1 Adjusted n to account for missing data. 2 Ever present. Abbreviations: LSHF (low symptoms/high function), HSBF (high symptoms/balanced function), MSBF (moderate symptoms, balanced function), HSPF (high symptoms/poor function
.jpg) Figure 1:Heatmap of clusters 1-4. Average values of each PRO measure are shown. PROMIS Ability to Participate and Physical Function values are subtracted from 100 to reflect reverse significance.
Figure 1:Heatmap of clusters 1-4. Average values of each PRO measure are shown. PROMIS Ability to Participate and Physical Function values are subtracted from 100 to reflect reverse significance.
.jpg) Figure 2: Alluvial plot demonstrating cluster attribution of individual patients over time.
Figure 2: Alluvial plot demonstrating cluster attribution of individual patients over time.
To cite this abstract in AMA style:
Grader-Beck T, Reed J, Patel P, Kim J, Baer A. Clustering by ESSPRI and PROMIS domain measures defines distinct subtypes and facilitates longitudinal assessment of patients with Sjogren’s disease [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/clustering-by-esspri-and-promis-domain-measures-defines-distinct-subtypes-and-facilitates-longitudinal-assessment-of-patients-with-sjogrens-disease/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/clustering-by-esspri-and-promis-domain-measures-defines-distinct-subtypes-and-facilitates-longitudinal-assessment-of-patients-with-sjogrens-disease/