Session Information
Date: Sunday, November 17, 2024
Title: Muscle Biology, Myositis & Myopathies – Basic & Clinical Science Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Diaphragmatic myositis is rarely reported in patients with idiopathic inflammatory myopathy (IIM) but is associated with high morbidity and mortality. Epidemiology, spectrum of clinical presentation, immunology, and treatment outcomes of these patients is unknown, since the available literature is limited to a few case reports/small case series mostly on inclusion body myositis (IBM). We report findings from a large cohort of (non-IBM) IIM patients with clinically significant diaphragmatic weakness.
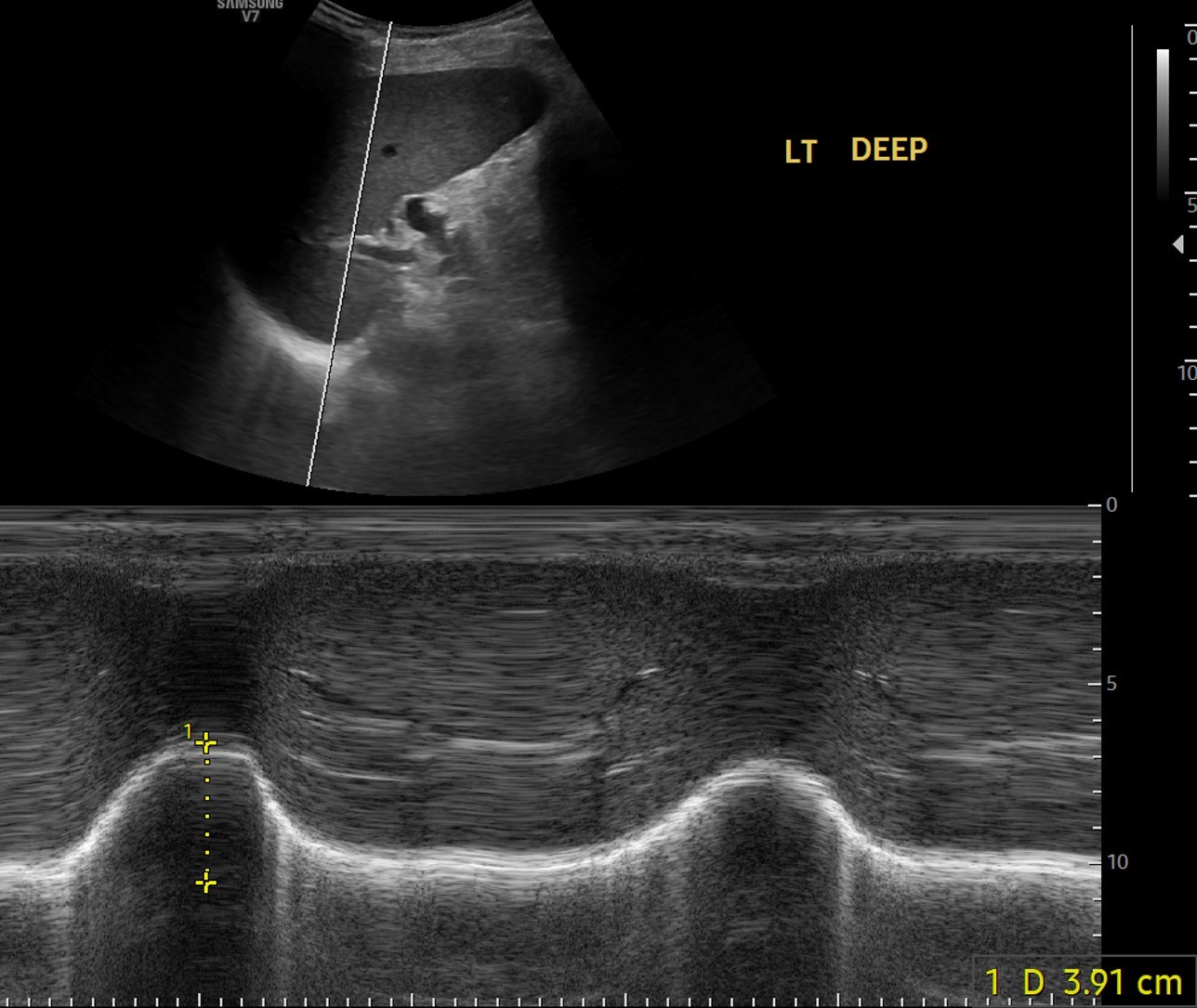
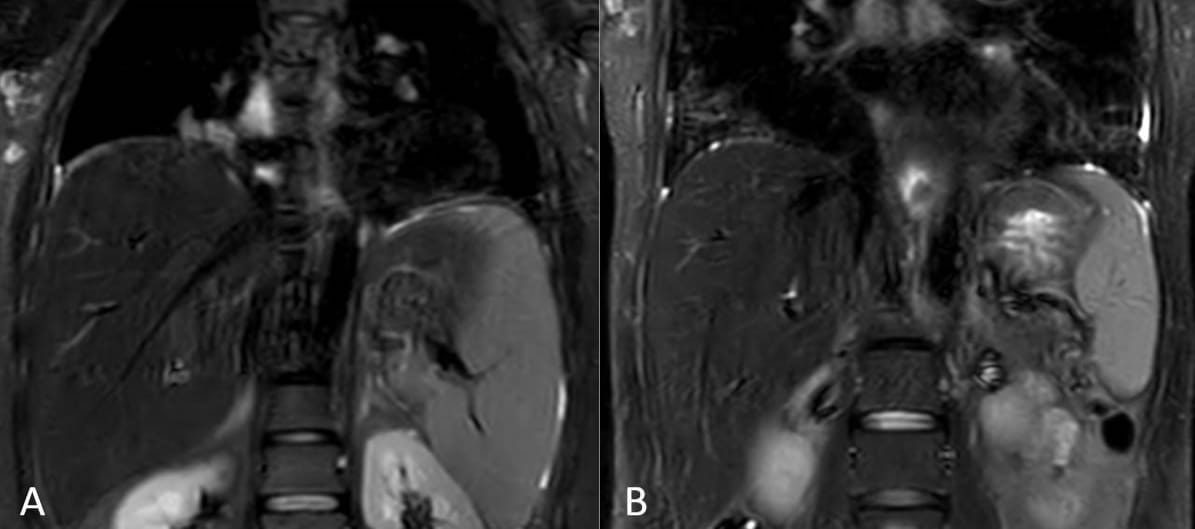
Methods: This single-center prospective cohort study included adult patients (>14 years) with IIM (non-IBM) admitted between Feb 2023 and June 2024 who had unexplained or disproportionate dyspnea, reduced single breath count, paradoxical breathing, or unexplained CO2 retention. Underlying diaphragmatic dysfunction was evaluated through diaphragmatic ultrasonography (DUS) (< 5cm excursion on deep breathing taken as diaphragmatic dysfunction) (Fig 1) or fluoroscopic sniff test (where DUS was unavailable). Evidence of diaphragmatic myositis on whole-body muscle MRI was also assessed, where available (Fig 2). These patients’ clinical and immunological profiles, treatment details, and outcomes were analyzed.
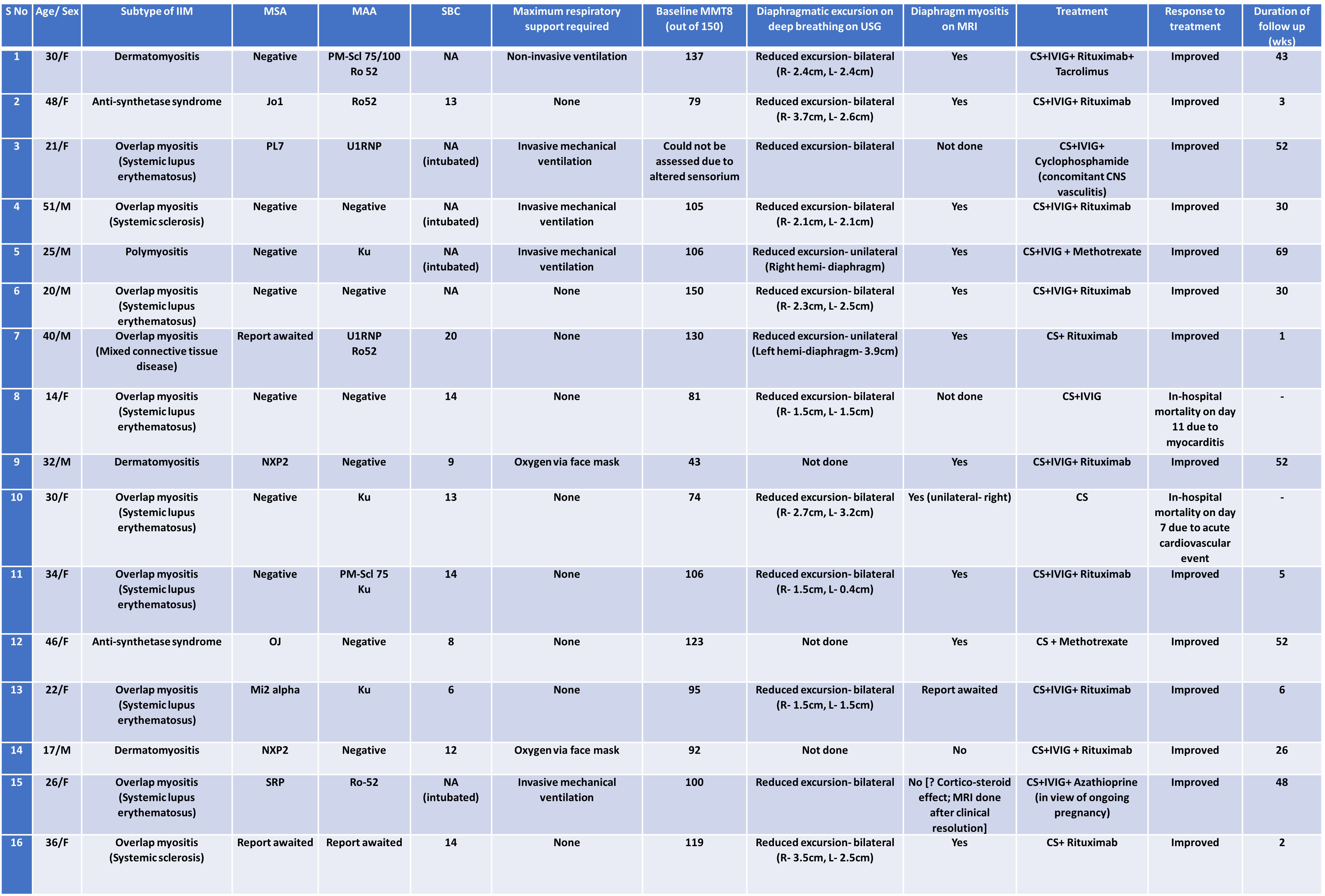
Results: Sixteen IIM patients [10 (62%) females, mean age 31(11) years] had clinically significant diaphragmatic weakness (Table 1). Most common IIM subtype was overlap myositis [10 (63%)], which was most commonly associated with lupus (60%); 3 (19%) had primary dermatomyositis, 2 antisynthetase syndrome, and 1 polymyositis. Clinical presentation was acute-subacute in 11(69%) patients. Five (31%) required ventilatory support [invasive mechanical ventilation in 4(80%)]; 2(12.5%) required transient oxygen support. Five (31%) patients had disproportionately severe diaphragmatic involvement with relatively preserved peripheral muscle strength, with one patient having isolated diaphragm involvement. The median MMT-8 score was 105 (43-150). Diaphragmatic excursion was reduced bilaterally in 11/14(79%) patients; 11/13(85%) had diaphragmatic myositis on MRI. 7/14 (50%) had myositis-specific antibody positivity (antisynthetase three, anti NXP2 two, one each of antiMi-2 and antiSRP); 9/15 (60%) had myositis-associated antibodies (most commonly anti-Ku and anti-Ro-52);3 were seronegative. Pulse steroids alone [4(25%)] or in combination with IVIG [12(75%)] were given as induction therapy, with which 14 (88%) patients improved and were discharged; two (12%) patients died in-hospital due to sudden cardiovascular events. Most commonly used steroid-sparing agent was rituximab [10(62%) patients]. The median duration of follow-up was 30(2-69) weeks.
Conclusion: Clinically significant diaphragmatic weakness in IIM is not uncommon, can occur acutely, in isolation, or as the dominant/first manifestation of underlying IIM, most commonly overlap myositis. Unexplained or disproportionate dyspnea should raise the suspicion of diaphragmatic involvement. DUS is a useful, non-invasive tool for rapid, bedside assessment in admitted patients. Prompt diagnosis and timely institution of aggressive immunosuppression can improve outcomes in this potentially fatal involvement.
To cite this abstract in AMA style:
Jain S, Pridhivi B, Khan A, Spalkit S, Soneja M, Sharma M, Sinha S, Kumar U, Wig N. Clinico-Immunological Profile and Treatment Outcomes of Clinically Significant Diaphragmatic Weakness in Patients with Idiopathic Inflammatory Myopathies: Results from the Largest Single-Center Cohort of 16 Cases [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/clinico-immunological-profile-and-treatment-outcomes-of-clinically-significant-diaphragmatic-weakness-in-patients-with-idiopathic-inflammatory-myopathies-results-from-the-largest-single-center-cohort/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/clinico-immunological-profile-and-treatment-outcomes-of-clinically-significant-diaphragmatic-weakness-in-patients-with-idiopathic-inflammatory-myopathies-results-from-the-largest-single-center-cohort/