Session Information
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Osteoarthritis (OA) is a leading cause of pain and disability in older adults marked by progressive joint degeneration. Symptom trajectories vary: some experience persistent limitations, while others improve. The Patient Acceptable Symptom State (PASS) provides a benchmark for meaningful symptom control, indicating when individuals report feeling well. We aimed to identify clinical phenotypes of people with radiographic OA (ROA) and symptoms who later achieve PASS. Such insights may allow identification of clinical factors to focus on for personalized OA care.
Methods: We used data from the Multicenter Osteoarthritis Study (MOST), a NIH-funded longitudinal cohort of people with or at risk of knee OA. ROA was defined as tibiofemoral (TF) Kellgren-Lawrence (KL) grade ≥2 and/or patellofemoral (PF) radiographic features. PASS was defined as Visual Analog Scale (VAS) pain ≤32.3 and WOMAC function ≤31.0 (0–100 scales). We began at the 30-month visit to minimize regression to the mean in pain and function scores. Eligible participants met two criteria: 1) ROA in at least one knee at 30 months; 2) not in PASS at 30 months who achieved PASS for both pain and function during follow-up up to the 16th year. We excluded those who had hyaluronic acid or steroid injections or joint replacement before achieving PASS. Variables used in clustering were age, BMI, sex, education, Center for Epidemiologic Studies Depression Scale (CES-D) score ≥16, VAS pain, WOMAC pain and function, medication use, KL grade, ROA location, prior knee surgery/injury, synovitis or cysts, bone mineral density (BMD), Charlson comorbidity index, Physical Activity Scale for the Elderly (PASE), and 20-meter walk time.
Principal components analysis (PCA) was used to reduce dimensionality and identify combinations of variables explaining the most variance. K-means clustering grouped participants into homogeneous subgroups. ANOVA and chi-square tests compared continuous and categorical variables across subgroups.
Results: Of 1,557 participants with ROA at 30 months, 446 were not in PASS; 121 later achieved PASS and were included in the cluster analysis. Figure 1 shows contributions of key variables to the first five principal components (PC1–PC5), which capture a large proportion of variance in the data. Thirteen components were needed to explain 80% of variance. We present in Table 1 the characteristics for the 3-cluster model due to its interpretability. Cluster 1 (n=55) reported the highest levels of pain and functional impairment, with the most severe disease (high proportion of KL grade 4 and whole knee ROA). Cluster 2 (n=57) had moderate symptoms and mixed radiographic severity in the TF joint. Cluster 3 (n=9) had mild symptoms, isolated PF ROA, and all participants were KL grade 1. Demographics, comorbidities, and physical characteristics were similar across clusters. Figure 2 plots PC1 and PC2, showing limited separation between clusters.
Conclusion: We identified three clusters that differed primarily by ROA severity and location. However, one cluster also had higher initial pain and worse function than the others demonstrating strong recovery.
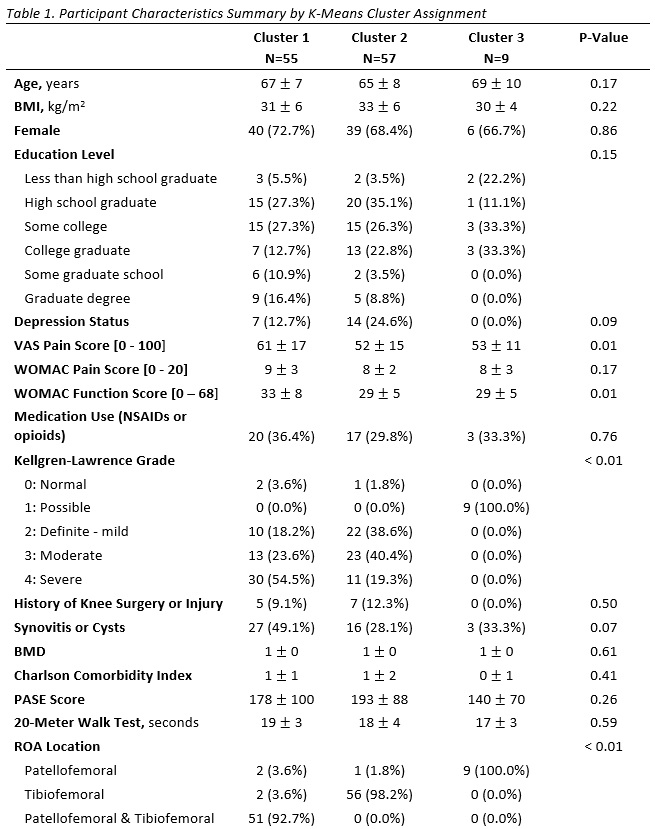 Continuous variables are summarized using mean ± SD, while categorical variables are summarized by the number of observations and percentages.
Continuous variables are summarized using mean ± SD, while categorical variables are summarized by the number of observations and percentages.
.jpg)
.jpg)
To cite this abstract in AMA style:
Tilley S, LaValley M, McGinley B, Lewis C, Torner J, Felson D, Neogi T. Clinical Phenotypes of Participants with Radiographic Osteoarthritis Attaining Patient Acceptable Symptom State in the Multicenter Osteoarthritis Study [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/clinical-phenotypes-of-participants-with-radiographic-osteoarthritis-attaining-patient-acceptable-symptom-state-in-the-multicenter-osteoarthritis-study/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/clinical-phenotypes-of-participants-with-radiographic-osteoarthritis-attaining-patient-acceptable-symptom-state-in-the-multicenter-osteoarthritis-study/