Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Diffuse alveolar hemorrhage (DAH) is a severe respiratory complication observed in certain rheumatic diseases, such as systemic lupus erythematosus (SLE), ANCA-associated vasculitides (AAV), and antiphospholipid syndrome (APS). This condition typically manifests over hours to days and has a high mortality rate. Coinfection can be present in these cases, but the implication in mortality is not well established.
We aimed to describe the clinical and infectious-related characteristics of patients with DAH associated with rheumatic diseases.
Methods: This was a cross-sectional and retrospective study from 2011 to May 2024. Demographic data, clinical presentation, laboratory findings, and microbiological characteristics were obtained from electronic medical records. DAH was diagnosed according to clinical, laboratory, imaging, and histopathological criteria, with preliminary classification criteria for SLE, AAV, and APS used as diagnostic tools. We used descriptive statistics to analyze coinfection vs. no-coinfection and intensive care unit (ICU) admission vs. non-ICU.
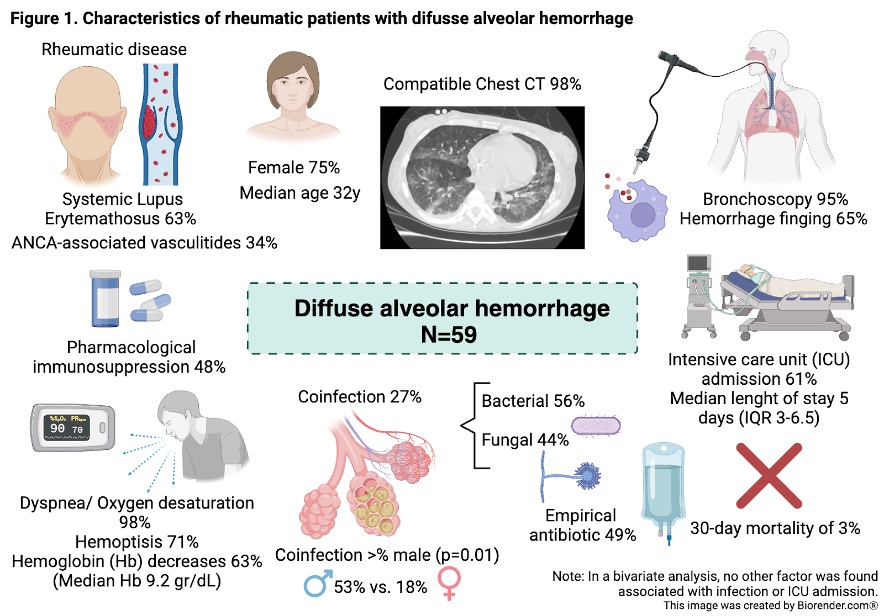
Results: Fifty-nine patients with DAH were included (figure); forty-for patients (75%) were females with a median age of 32 years (IRQ:24-44); SLE (63%) and ANCA-associated vasculitides (34%) were the most frequent rheumatologic diseases; 54% (n=32) had another comorbidity, CKD (24%) and HBP (20%) were the most frequent. At the time of admission, 28 patients (48%) were using immunosuppressive drugs, the most frequent was cyclophosphamide in 21%, and 19 patients (32%) were using prednisone with a median dose of 20 mg/day.
Thirty-six patients (61%) had identified another disease activity; the most frequent activity was renal in 61%. The majority (98%) had imaging studies consistent with DAH, hemoptysis (71%), and bronchoalveolar lavage findings consistent with DAH (61%). The treatment was pulse methylprednisolone in fifty-six patients (95%). Thirty-six patients (61%) required admission to the ICU; no differences were found between the groups.
Forty-nine patients (83%) received empirical antibiotic therapy upon presentation. Beta-lactams were the most frequently used antibiotics, and piperacillin/tazobactam was the most common choice. It was administered to 31 of 49 patients (63.3%). Thirty-nine patients (79.6%) received dual coverage, with vancomycin being the most often employed (28/49, 57.1%), followed by clarithromycin (9/49, 18.4%). The mean days of antibiotic therapy was 6.2 (SD4). Microbiological diagnoses were obtained in 16 out of 59 patients (27%), with bacteria identified in 9/16 cases (56%) and fungi in 7/16 cases (44%). There were two reported deaths (3%), both of which were due to causes unrelated to DAH.
Conclusion: Mortality was lower than previously reported in the literature, possibly related to early treatment. Coinfection was present in a third of patients, more frequent in males. Invasive fungal infections were found in a relevant percentage of the cases, so a targeted treatment is needed.
To cite this abstract in AMA style:
Briones-García E, Navarro-Lara S, Ortiz-Bustamante M, García Herrera I, Roman-Montes C, Guaracha-Basañez G. Characteristics and Coinfections of Diffuse Alveolar Hemorrhage in Rheumatic Patients [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/characteristics-and-coinfections-of-diffuse-alveolar-hemorrhage-in-rheumatic-patients/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/characteristics-and-coinfections-of-diffuse-alveolar-hemorrhage-in-rheumatic-patients/