Session Information
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: RA patients have at least twice the risk of CVD. In fact, CVD is the leading cause of morbidity and premature mortality in RA. Inflammation driven endothelial dysfunction leads to accelerated atherosclerosis and premature CVD in RA. JAKi, tofacitinib, in human aortic endothelial culture inhibits VCAM-1, ICAM-1, TNF-a, IL-1b. However, tofacitinib increases MACE risk in RA patients with ASCVD.
Impact of Tofacitinib on endothelial function in RA patients with inadequate response to csDMARDs in the absence of conventional CV risk factors or pre-existing CVD needs exploration. Endothelial dysfunction (ED), the ” sine qua non” for atherosclerosis appearance, is the key promoter of CVD. ED is a barometer for CV health and a seminal target for reducing cardiovascular (CV) risk in RA.
The objective was to prospectively investigate the impact of Tofacitinib (TOFA) on CV risk in active RA in absence of overt CVD or its risk factors.
Methods: 81 consecutive RA patients meeting 2010 Rheumatoid Arthritis Classification Criteria median age 54 years, 81% female, disease duration 14 years, moderate to high activity (DAS28-5.3) who were non-responders to MTX at least 15 mg/week and/or other synthetic DMARDs free of clinical overt cardiovascular disease were randomized 1:1 to receive TOFA 5 mg bid (n=41) or placebo (n=41) for 12 weeks as an adjunct to existing stable antirheumatic drugs. Primary endpoints included endothelial dysfunction assessed by FMD, using Angiodefender, at baseline and after 12 weeks of treatment and occurrence of MACE and VTE throughout the study. The secondary end points included: DAS28, ESR, CRP, HAQ-DI. .
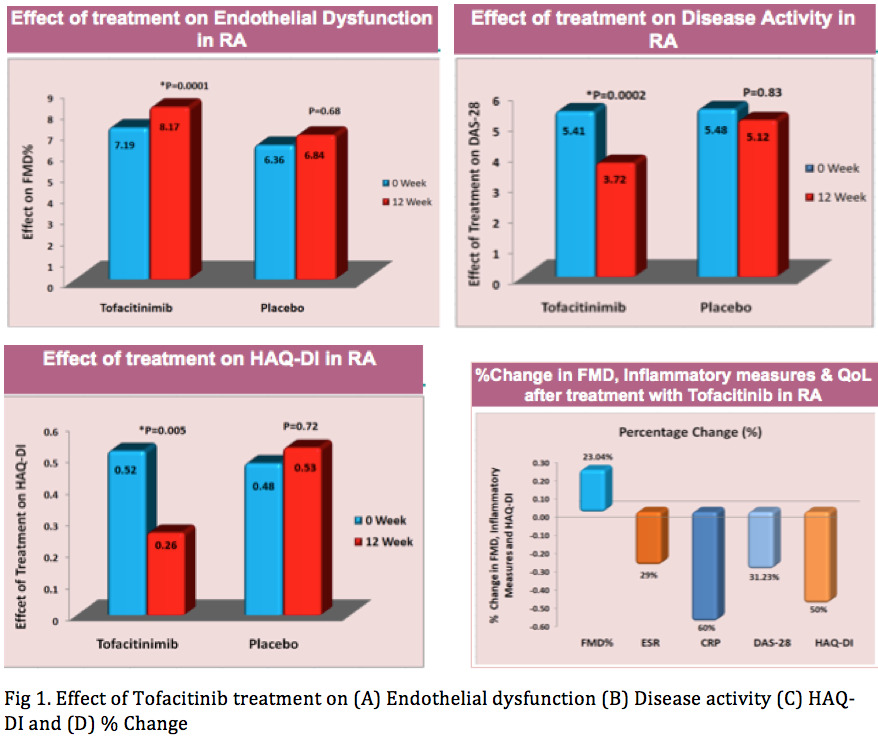
Results: At baseline, endothelial function was impaired and levels of inflammatory measures were elevated and HAQ-DI was impaired in both groups. After treatment, FMD improved significantly in the tofacitinib group from (6.64 ± 2.13 to 8.17 ± 2.69, p=0.0001) as compared to placebo (6.36 ± 3.01% to 6.84 ± 2.95%, p=0.68) (Fig. 1A). DAS28 (Fig. 1B), ESR and CRP levels improved significantly in tofacitinib group as compared to placebo (p≤0.05). TOFA significantly decreased HAQ-DI (Fig. 1C) values as compared to placebo. There was no MACE or VTE event during the study period in either group. After 12 weeks of treatment, FMD increased by 23.04% where as DAS28, ESR and CRP decreased by 31.23%, 29% and 60% respectively in the TOFA group (Fig 1D). Significant negative correlation was observed between FMD and CRP (0.32, p≤0.05) before and after (r= -0.34, p≤0.05) treatment with TOFA whereas no such correlations were found in placebo group.
Conclusion: TOFA, apart from its anti-inflammatory activity, improves endothelial dysfunction and cardiovascular risk in active RA without clinical overt cardiovascular disease. Thus, JAK inhibition with TOFA has vasculoprotective and cardioprotective effect mediated through anti-inflammatory and probably other mechanisms.
To cite this abstract in AMA style:
Syngle A, verma I, Garg N, Chauhan K, Patyal S, Syngle D. Cardioprotective Impact of JAKi, Tofacitinib, on CV Risk in Rheumatoid Arthritis: JAKi CV Risk Impact Study [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/cardioprotective-impact-of-jaki-tofacitinib-on-cv-risk-in-rheumatoid-arthritis-jaki-cv-risk-impact-study/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/cardioprotective-impact-of-jaki-tofacitinib-on-cv-risk-in-rheumatoid-arthritis-jaki-cv-risk-impact-study/