Session Information
Date: Tuesday, October 28, 2025
Title: (1972–1989) Measures & Measurement of Healthcare Quality Poster II
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Patients with rheumatologic conditions who are on immunosuppressive therapy face an elevated risk of pneumococcal infections, particularly those in medically underserved populations. Per ACR and recent CDC guidelines, pneumococcal vaccination is recommended for immunocompromised adults under age 65 and, more recently, for those aged 19–49. However, in busy outpatient settings, vaccination is frequently overlooked. Our goal is to increase pneumococcal vaccination rates among immunocompromised rheumatology patients from a baseline of 33% to 50% in 3 months at North East Medical Services (NEMS), a federally qualified health center (FQHC).
Methods: We focused on patients under 65 years of age diagnosed with RA, PsA, AS, or SLE who were receiving immunosuppressive therapy (excluding hydroxychloroquine and sulfasalazine monotherapy). We used the prior age cutoff (< 65) as the updated CDC guideline for adults under 50 was only released in October 2024 and likely has had limited impact so far. From September 2024 to January 2025, the baseline vaccination rate was identified as 33%. We considered a variety of pneumococcal vaccination sequences valid, including PCV20 or PCV21 alone, PPSV23 followed by PCV20 or PCV21, and PCV13 followed by PCV20 or PCV21.A root cause analysis (Figure 1) revealed key barriers: patient, physician and other departments (eg, pharmacy, dental). To address these, we introduced a bilingual patient education flyer (English and Mandarin, Figure 2) distributed across all NEMS clinics, simplified the vaccine protocol to PCV20 only, and implemented EMR-based care gap alerts. Additionally, a blast email was sent to all NEMS providers, including PCPs, specialists, and dental staff. The initiative was highlighted during our monthly Medical Quality meeting. At the 2-month mark, we also engaged the pharmacy department to review patients’ medication and problem lists during dispensing and offer vaccination if not offered already during clinic visits..
Results: Between September 2024 and January 2025, 109 patients under 65 with RA, PsA, AS, or SLE were seen in the NEMS rheumatology clinic. At baseline, 36 patients (33%) had received a pneumococcal vaccine. By the two-month checkpoint, the rate had increased to 42%, still short of our 50% target. In response, we strengthened collaboration with the pharmacy department, emphasizing their role in reviewing patient records and administering missed vaccinations. This effort led to a continued rise in coverage, and after three months of intervention (February to May 2025), the vaccination rate increased from 33% to 50%, successfully reaching our goal.
Conclusion: Patients with rheumatologic diseases are at increased risk of pneumococcal infection, particularly those in underserved communities. By implementing targeted interventions such as patient education, provider reminders, streamlined EMR alerts, and pharmacy engagement, we successfully reached our vaccination rate goal. With a longer intervention period, we believe coverage could improve even further. This quality improvement model can also be adapted for other types of vaccines and high-risk populations, offering a sustainable strategy to reduce disparities in preventive care.
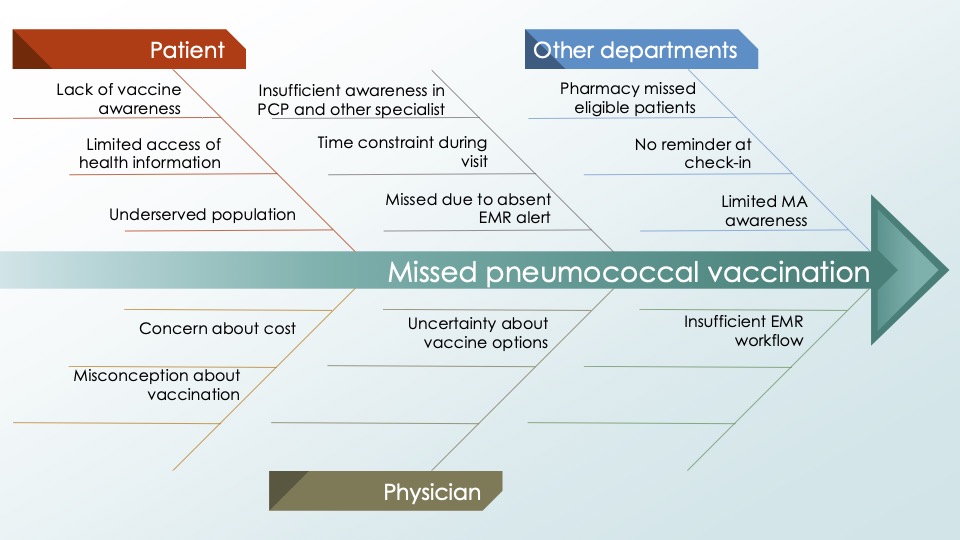 Figure 1: Root cause analysis identified key barriers across three main areas—patients, physicians, and other departments
Figure 1: Root cause analysis identified key barriers across three main areas—patients, physicians, and other departments
.jpg) Figure 2: Patient education flyer (in English and Mandarin) on pneumococcal vaccination for immunocompromised individuals with rheumatologic conditions
Figure 2: Patient education flyer (in English and Mandarin) on pneumococcal vaccination for immunocompromised individuals with rheumatologic conditions
.jpg) Table 1: Comparison of vaccination rates and patient demographics at baseline and after intervention
Table 1: Comparison of vaccination rates and patient demographics at baseline and after intervention
To cite this abstract in AMA style:
Lin K, Hao Y, Abdelnabi M, Lam W. Bridging the Gap in Underserved Care: A Quality Improvement Initiative to Increase Pneumococcal Vaccination Rates in Immunocompromised Rheumatology Patients [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/bridging-the-gap-in-underserved-care-a-quality-improvement-initiative-to-increase-pneumococcal-vaccination-rates-in-immunocompromised-rheumatology-patients/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/bridging-the-gap-in-underserved-care-a-quality-improvement-initiative-to-increase-pneumococcal-vaccination-rates-in-immunocompromised-rheumatology-patients/