Session Information
Date: Monday, November 14, 2022
Title: Abstracts: Systemic Sclerosis and Related Disorders – Clinical II: Clinical Phenotypes
Session Type: Abstract Session
Session Time: 9:00AM-10:30AM
Background/Purpose: We sought to examine the association between anti-Sjögren syndrome/scleroderma autoantigen 1 (SSSCA1) antibody and cancer in systemic sclerosis (SSc). We also describe the frequency of anti-SSSCA1 antibody positivity and associated clinical phenotype in patients with SSc.
Methods: We conducted a case-control study using data from 210 patients with SSc and cancer, and 205 SSc patients without cancer. All were randomly selected from the Johns Hopkins Scleroderma Center Research Registry. Antibodies against SSSCA1 were assayed by immunoprecipitation of 35S-methionine-labeled protein generated by in vitro transcription and translation. We performed logistic regression analysis to examine the relationship between anti-SSSCA1 antibodies and cancer.
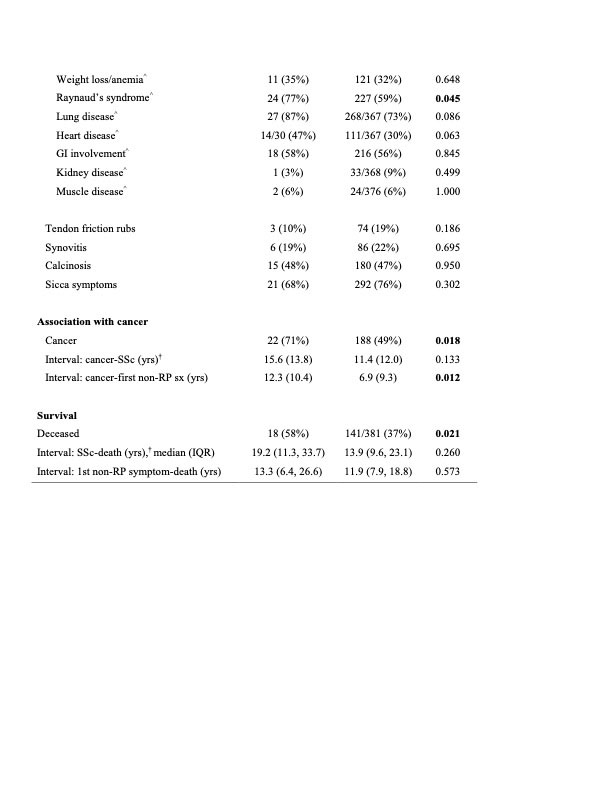
Results: Among the 415 study patients, 31 (7%) were anti-SSSCA1-antibody positive. Patients with cancer were significantly more likely to be anti-SSSCA1 positive compared to those without cancer (22/210 [10%] vs. 9/205 [4%], respectively; p=0.018). After adjusting for age at SSc onset, sex, race, cutaneous subtype, follow up time and a history of smoking, patients with anti-SSSCA1 antibodies had an increased risk of cancer (OR 2.37, 95% CI 1.03, 5.46) compared to anti-SSSCA1-negative patients. Antibody-positive patients were more likely to have severe Raynaud’s phenomenon, a lower minimum ejection fraction, a trend toward more severe heart involvement (defined by arrhythmia, left ventricular EF< 45% or clinical signs of heart failure), and a lower baseline DLCO percent predicted than anti-SSSCA1-negative patients.
Conclusion: These data suggest anti-SSSCA1 antibody status serves as a biomarker for cancer in patients with SSc. Anti-SSSCA1 positive patients with SSc may be more likely to have severe Raynaud’s and cardiac involvement.
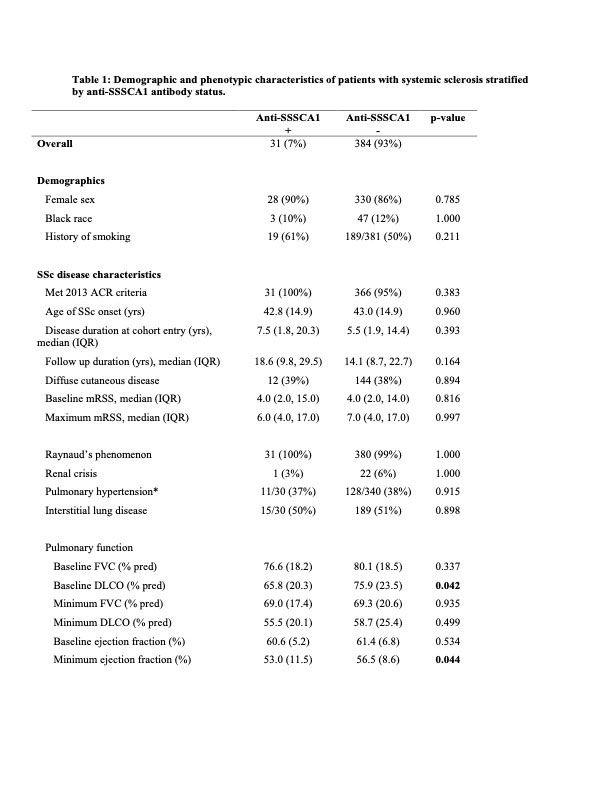
A p-value in bold indicates a statistically significant difference between anti-SSSCA1+ and anti-SSSCA1-
Unless otherwise stated, values represent whether the manifestation has ever emerged or maximal disease severity over the course of follow up.
Abbreviations: ACR: American College of Rheumatology; DLCO: diffusing capacity of the lungs for carbon monoxide; FVC= forced vital capacity; GI = gastrointestinal; IQR = interquartile range; mRSS = modified Rodnan skin score; no. = number; pred = predicted; RP=Raynaud’s phenomenon; SD = standard deviation; SSc = systemic sclerosis; sx: symptom
Explanations:
*Pulmonary hypertension defined by estimated right ventricular systolic pressure (RVSP) ≥45 mmHg on echocardiogram.
^ Moderate-severe disease: weight loss/anemia = weight loss ≥ 10.0 kg or hematocrit ≤ 32.9; Raynaud’s syndrome = digital pits, ulceration or gangrene; lung = FVC and/or DLCO <70% predicted, mild-severe PH or oxygen dependence; heart = left ventricular ejection fraction < 45%, clinical signs of left or right heart failure or sustained clinically important arrhythmia; GI = high dose acid reflux medications, antibiotics for bacterial overgrowth, malabsorption syndrome, episodes of pseudo-obstruction or total parental nutrition requirement; kidney = serum creatinine ≥ 1.7 mg/dL, or at least 2+ urine protein; muscle = strength of ≤ 3/5 in upper or lower extremities, or requirement of ambulatory aids.
†SSc onset is defined as date of Raynaud’s phenomenon or non-Raynaud’s phenomenon symptom, whichever was first. Positive values denote cancer diagnosis after SSc onset, and negative values indicate cancer preceding SSc onset.
To cite this abstract in AMA style:
Wallwork R, Casciola-Rosen L, Shah A. Association Between Anti-Sjögren Syndrome/Scleroderma Autoantigen 1 (SSSCA1) Antibodies and Cancer in Systemic Sclerosis [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/association-between-anti-sjo%cc%88gren-syndrome-scleroderma-autoantigen-1-sssca1-antibodies-and-cancer-in-systemic-sclerosis/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/association-between-anti-sjo%cc%88gren-syndrome-scleroderma-autoantigen-1-sssca1-antibodies-and-cancer-in-systemic-sclerosis/