Session Information
Date: Saturday, November 16, 2024
Title: SpA Including PsA – Diagnosis, Manifestations, & Outcomes Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: The SARC-F is a self-report screening tool for sarcopenia (Sar) used to identify individuals at risk for poor functional outcomes [1]. The aim of this study was to evaluate the association of SARC-F with disease activity, functional muscle status, patient-reported outcome (PRO) and body composition in patients with axial spondyloarthritis (axSpA) and psoriatic arthritis (PsA).
Methods: Patient and disease characteristics, disease activity, Short Physical Performance Battery (SPPB), gait speed, hand grip strength, Patient’s global assessment (PGA), Short Questionnaire to Assess Health-enhancing physical activity (mSQUASH) and body composition parameters by DXA (fat mass (FM) index (FMI) and appendicular lean mass (ALM) index (ALMI)) were measured. Variables were compared between those with a SARC-F score ≥4 and < 4, higher values indicating increased likelihood of Sar. Obesity was defined by DXA body fat percentage ≥30% (male) or ≥40% (female) patients and sarcopenia by ALM/BMI according to the FNIH (Foundation of the National Institutes of Health) definition (< 0.789 (male) or < 0.512 (female)). Patients with Sar and obesity were classified as sarcopenic obese. Linear regression analyses were used to examine the association between Sar and various patients’ characteristics additionally adjusted for potential confounders (age, sex).
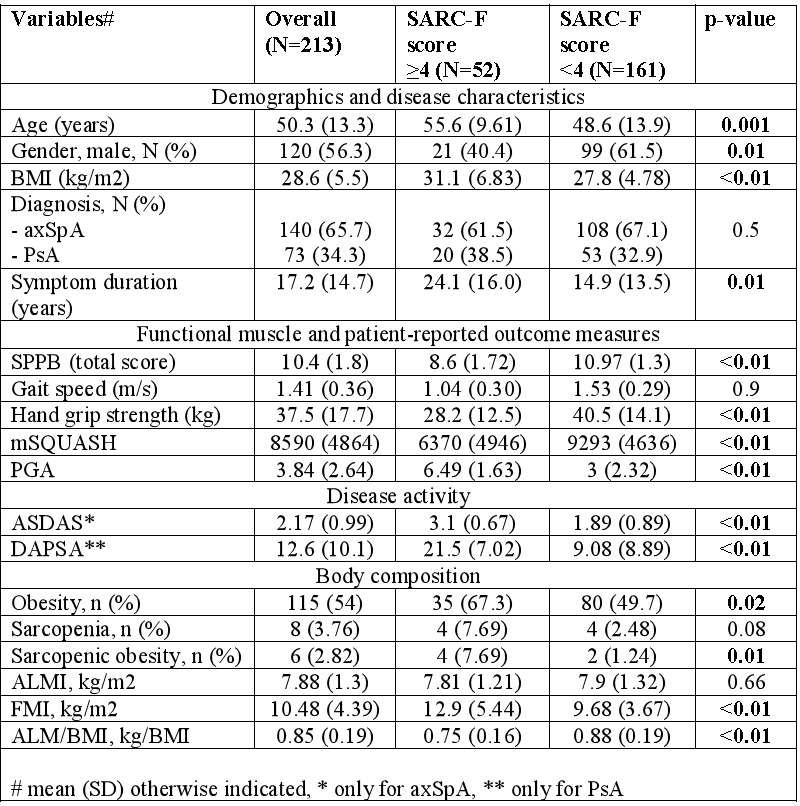
Results: A total of 213 SpA patients (140 (65.7%) axSpA and 73 (34.3%) PsA) were included (table 1). A total of 127 patients were treated with bDMARDs (59.6%) and 62 with NSAIDs or csDMARDs (29.1%). Fifty-two (24.4%) patients had a SARC-F score ≥4. Patients with SARC-F ≥4 were older, more often female, obese and sarcopenic obese, had longer symptom duration and higher disease activity scores. SPPB, hand grip strength, and mSQUASH values were significantly lower and PGA was significantly higher in patients with SARC-F ≥4 but gait speed was not different between groups. Prevalence of Sar was numerically higher in patients with SARC-F ≥4 compared to SARC-F < 4 (7.7 versus 2.5%), while ALM/BMI index was significantly lower and FMI significantly higher in patients with SARC-F ≥4.
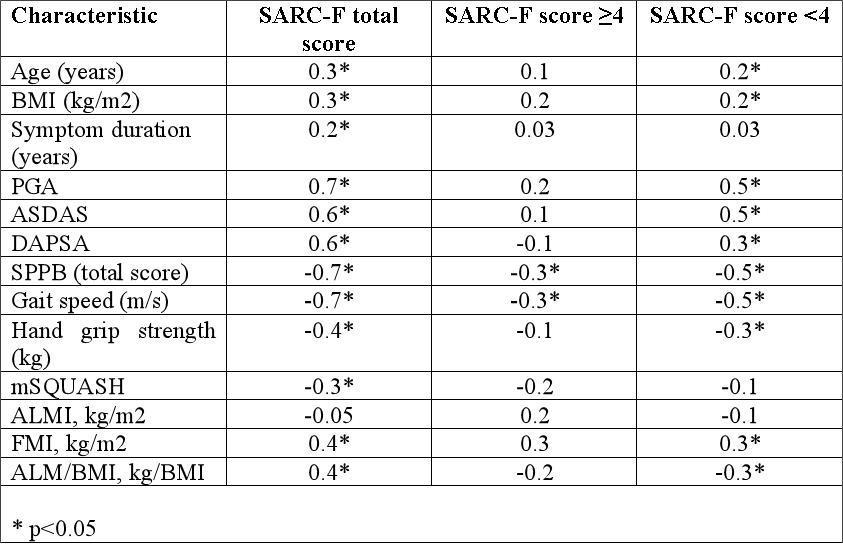
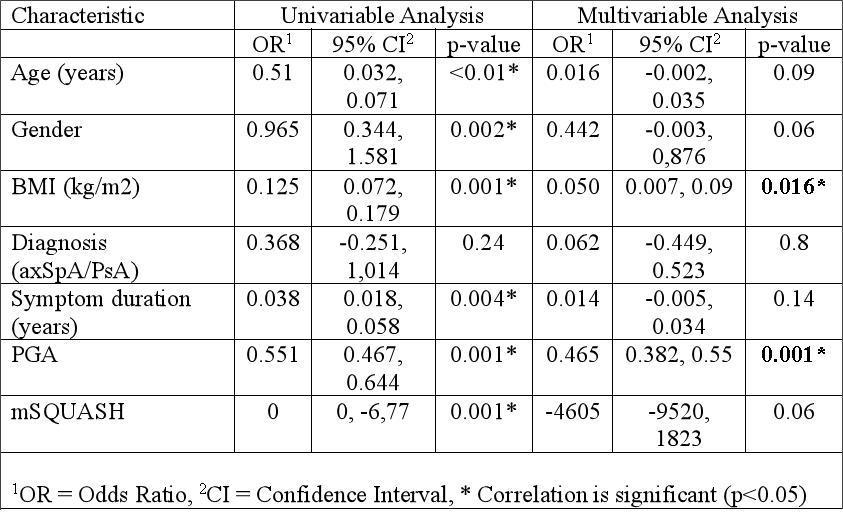
Both total SARC-F score and SARC-F score < 4 significantly correlated with disease activity, functional muscle status, PRO and DXA, except symptom duration and mSQUASH with SARC-F score < 4, and except ALMI with all SARC-F components (table 2). While SARC-F score ≥4 correlated weakly only with SPPB and gait speed (r=0.28). Obesity and PGA were associated with higher odds of SARC-F ≥4 (table 3).
Conclusion: We report a significant association of the SARC-F with disease activity and functional muscle status measures. Importantly, the SARC-F questionnaire did not differentiate between patients with and without sarcopenia based on the FNIH definition. Further research is needed to explore if this might be due to the small sample size of this study or if the SARC-F has limitations to screen for sarcopenia in patients with rheumatic diseases.
References:
1. Malmstrom TK et al. J Cachexia Sarcopenia Muscle 2016;7:28-36.
To cite this abstract in AMA style:
Kononenko I, Bedei M, Buehring B, Baraliakos X, Kiltz U. Association Between a Self-Report Screening Tool for Sarcopenia (SARC-F) and Disease Activity, Muscle Strength and Muscle Power Measures, Patient-Reported Outcomes and Body Composition in Patients with Spondyloarthritides [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/association-between-a-self-report-screening-tool-for-sarcopenia-sarc-f-and-disease-activity-muscle-strength-and-muscle-power-measures-patient-reported-outcomes-and-body-composition-in-patients-wit/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/association-between-a-self-report-screening-tool-for-sarcopenia-sarc-f-and-disease-activity-muscle-strength-and-muscle-power-measures-patient-reported-outcomes-and-body-composition-in-patients-wit/