Session Information
Date: Monday, November 14, 2022
Title: Metabolic and Crystal Arthropathies – Basic and Clinical Science Poster
Session Type: Poster Session D
Session Time: 1:00PM-3:00PM
Background/Purpose: Gout is the most common inflammatory arthritis, caused by hyperuricemia and subsequent deposition of aggregated monosodium urate (MSU) crystals in both articular and extra-articular regions. A strong association exists between hyperuricemia, gout and risk of cardiovascular disease. CT (DECT) has been shown to detect MSU deposition in vasculature of gout patients with correlation of tophus volume with cardiovascular risk. Vascular Positron Emission Tomography (PET/CT) has been extensively validated to measure arterial vessel wall inflammation. We postulate that uric acid deposits in the vasculature may cause local vascular inflammation. This could be a mechanism involved in theprogression of atherosclerosis and facilitate early onset of adverse cardiovascular events.
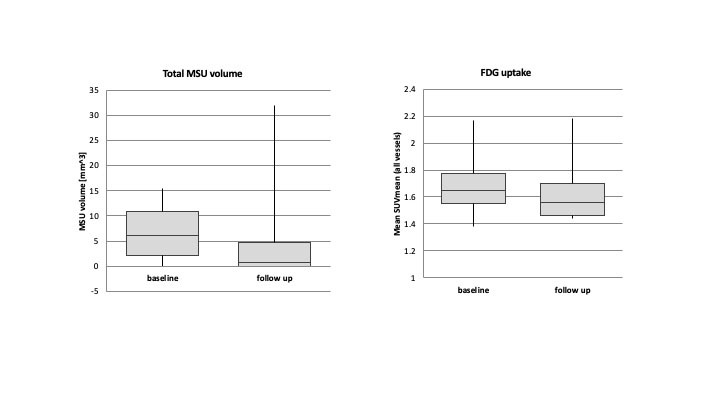
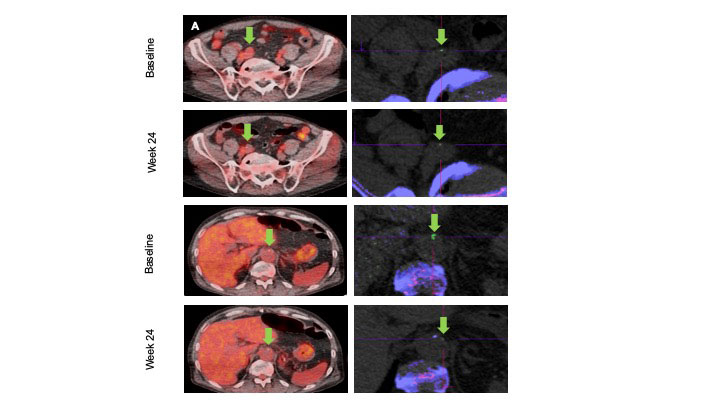
Methods: Ten patients with tophaceous gout who were either intolerant or refractory to urate lowering therapy were recruited. Patients were pre-treated with low dose immunomodulator (Azathioprine or Methotrexate) to prevent formation of anti-pegloticase antibodies and then were treated with pegloticase infusions every two weeks for 6 months. DECT and PET/CT were done at baseline and after 6 months of pegloticase to detect vascular MSU deposition (MSU volume) and vessel wall inflammation (Standard uptake value, SUV mean to assess systemic uptake across a vessel segment, SUV max to identify hotspots; Target-to-blood pool ratio, TBR mean and TBR max calculated by dividing the vascular wall SUV with the venous blood pool SUV mean, to correct for blood uptake) respectively. Data were summarized using means and standard deviations. Comparisons of the baseline and follow-up values were conducted for each variable using mixed effect models.
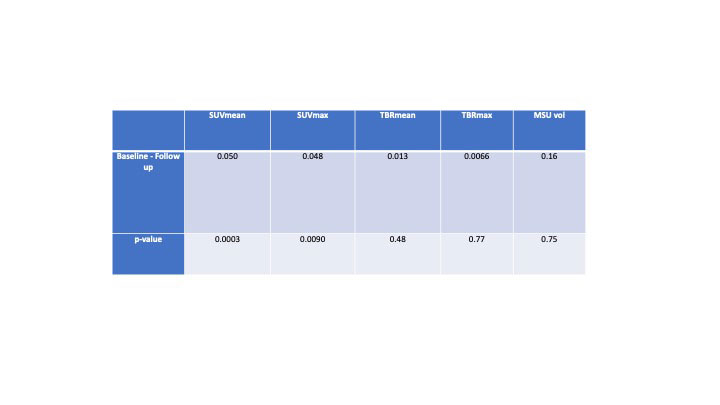
Results: We found a statistically significant decrease in SUV mean (p=0.0003) and SUV max (p=0.0090) across all arteries studied after treatment with pegloticase. There was a trend for decrease in TBR mean and TBR max, which was not statistically significant. In terms of MSU deposition, we found a trend for decrease in MSU volume after treatment with pegloticase, which was not statistically significant.
Conclusion: We observed a statistically significant reduction in vessel wall inflammation (SUV mean and SUV max) along with a trend towards a decrease in MSU deposition (MSU volume) in tophaceous gout patients following treatment with pegloticase. Despite the small sample size of our study, we were able to demonstrate a decrease in both vessel wall inflammation and MSU deposition by aggressively lowering uric acid. These findings suggest a role of MSU in vascular inflammation and demonstrate a concomitant decrease in vessel inflammation as the serum urate level is depleted. It remains to be seen if this correlates to a decrease in adverse cardiovascular outcome.
To cite this abstract in AMA style:
Khanna I, Mani V, Pyzik R, Kaufman A, Chi W, Bagiella E, Robson P, Ali Y. Assessing Urate Deposition and Inflammation in the Vasculature of Gout Patients Using Dual Energy Computed Tomography and Positron Emission Tomography Pre and Post Pegloticase- a Pilot Study [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/assessing-urate-deposition-and-inflammation-in-the-vasculature-of-gout-patients-using-dual-energy-computed-tomography-and-positron-emission-tomography-pre-and-post-pegloticase-a-pilot-study/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/assessing-urate-deposition-and-inflammation-in-the-vasculature-of-gout-patients-using-dual-energy-computed-tomography-and-positron-emission-tomography-pre-and-post-pegloticase-a-pilot-study/