Session Information
Session Type: Poster Session B
Session Time: 9:00AM-10:30AM
Background/Purpose: Fibromyalgia (FM) and depression (DEP) are common comorbidities of all reported primary rheumatic diagnoses, easily recognized in many patients, but often underestimated, particularly in patients who meet criteria for a primary rheumatic disease. Two screening indices to recognize FM and/or DEP are found within a 2-page multidimensional health assessment questionnaire (MDHAQ), FAST4 (fibromyalgia assessment screening tool) and MDS2 (MDHAQ depression screen). FAST4 agrees 90% with 2011 revised FM criteria, and MDS2 agrees 80% with reference HADS-D (hospital anxiety and depression scale–DEP). We analyzed the proportion of patients with various diagnoses seen in routine rheumatology care who screened positive or negative for FM or DEP according to FAST4 or MDS2 and reference 2011 FM Criteria or HADS-D.
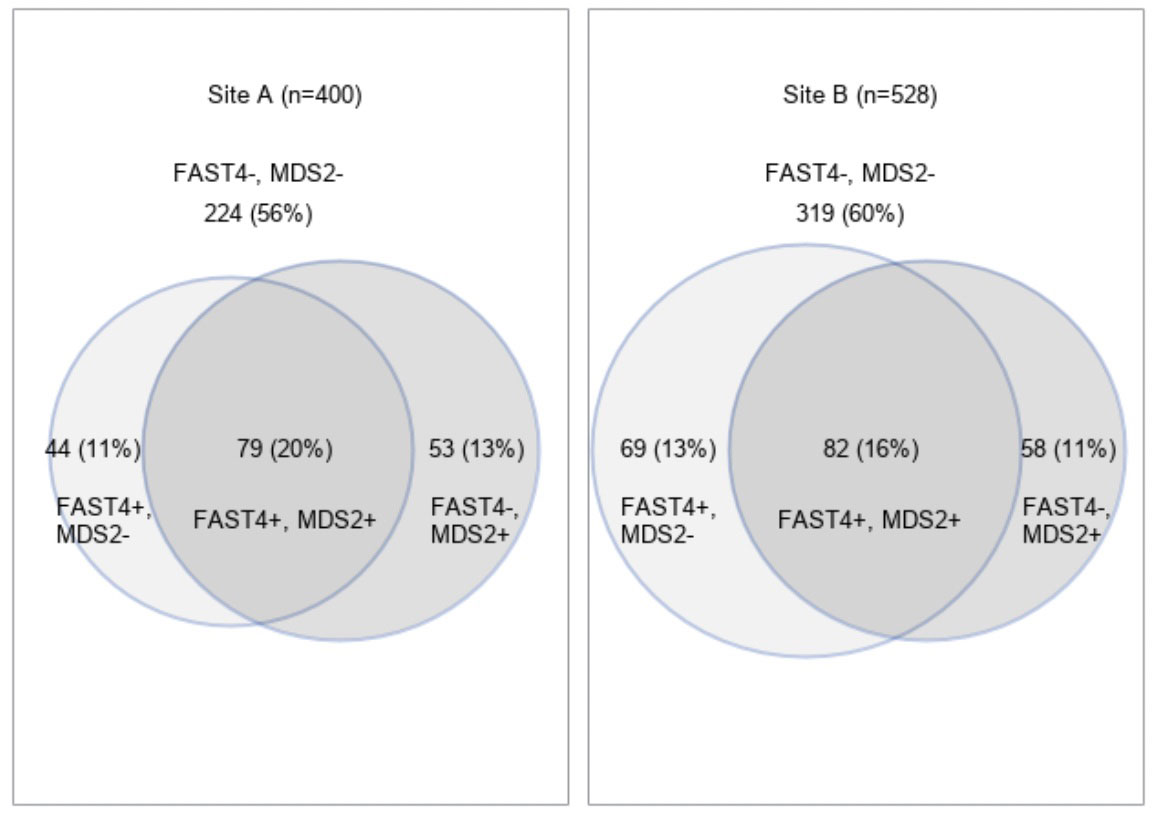
Methods: The MDHAQ is a 2-page patient self-report questionnaire designed for routine care, completed by most patients with all diagnoses in 5-10 minutes at all visits to 2 rheumatology sites. The MDHAQ includes a 0-10 pain VNS, 0-10 fatigue VNS, 0-3.3 DEP query, patient self-report 0-54 painful joint score, 60-symptom checklist including DEP, medical history queries, and FAST4 and MDS2 indices. FAST4 indicates FM if 3/4 of: pain VNS ≥6/10, fatigue VNS ≥6/10, self-report painful joint count ≥16/54, and/or symptom checklist ≥16/60. MDS2 indicates DEP if 0-3.3 DEP query response is ≥2.2 OR DEP is checked on the symptom checklist. The percent of patients with various primary diagnoses who were positive for FAST4, MDS2, 2011 FM revised criteria, or HADS-D was computed, including a Venn diagram for the proportions of all patients who were FAST4+/MDS2-, FAST4-/MDS2+, and FAST4+/MDS2+ at the 2 sites.
Results: Among 1,038 routine rheumatology care patients, 28.0% had an ICD-10 primary diagnosis of rheumatoid arthritis (RA), 12.6% osteoarthritis (OA), 6.3% primary FM, 42.0% inflammatory diagnoses other than RA and 11.1% noninflammatory diagnoses other than OA or primary FM (Table). FM 2011 revised criteria were met by 28.4% of patients, FAST4 positivity by 29.6%, HADS-D positivity by 35.1%, and MDS2 positivity by 28.6%, similar to RA, the most prevalent primary diagnosis. FM and DEP positivity according to MDHAQ indices or reference criteria were higher in OA and other non-inflammatory diseases than in RA and other inflammatory diseases, although the percent for all diagnosis categories were within 12% of all diagnoses except for FM in primary FM (Table). The Figure indicates that 11-13% of all patients were positive only for FM, 11-13% positive for only DEP, and 16-20% positive for both FM and DEP. Of patients positive for FM or DEP, about 29% were positive for either FM or DEP and 42% for both FM and DEP
Conclusion: The prevalence of FM or DEP in rheumatology patients is as high as for any primary diagnosis at these 2 rheumatology sites, feasibly recognized by FAST4 and MDS2 on an MDHAQ completed by most patients in 5-10 minutes. FM and/or DEP may confound assessment of clinical status and explain poor treatment responses in many patients.
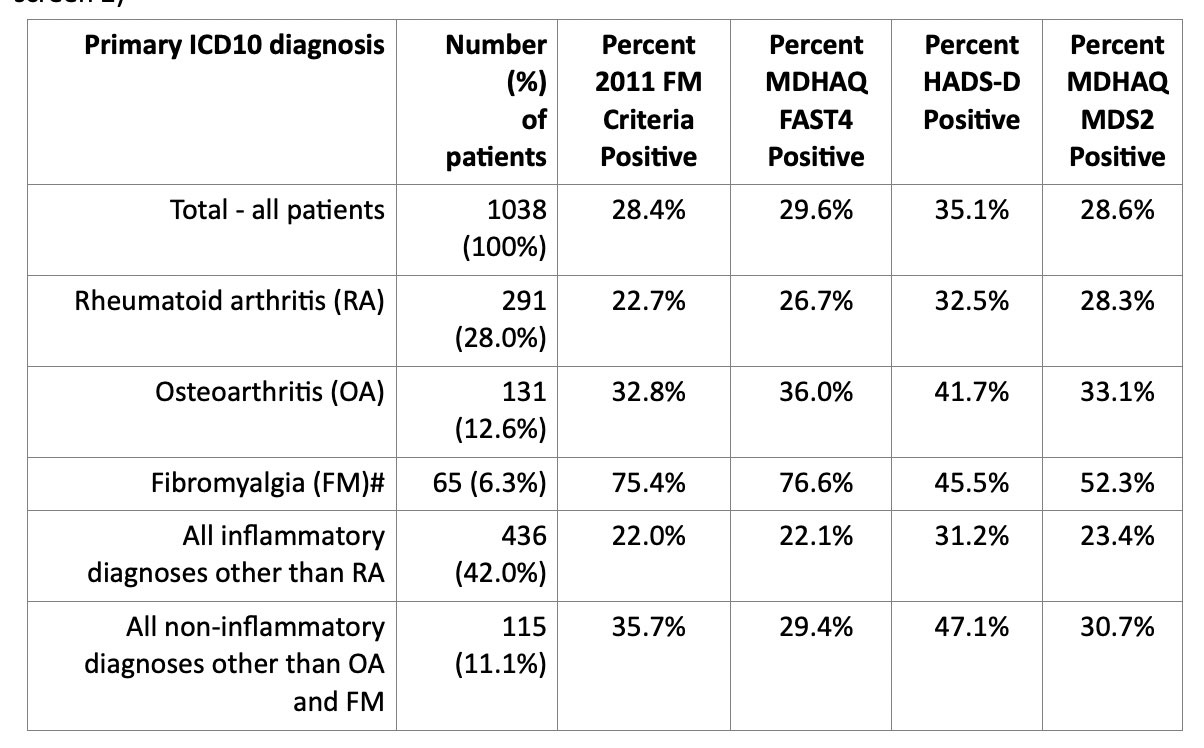
*The denominator is the total number of patients in the header of the column. The denominator for percentages in other columns is the total observations with non-missing specific variables for each row.
# Fibromyalgia is according to primary physician diagnosis.
To cite this abstract in AMA style:
Pincus T, Gibson K, Schmukler J, Li T, Block J. Are Fibromyalgia and Depression as Common as Any Primary Diagnosis in Routine Rheumatology Care, Albeit as Secondary Diagnoses, but Which May Confound Clinical Assessment? [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/are-fibromyalgia-and-depression-as-common-as-any-primary-diagnosis-in-routine-rheumatology-care-albeit-as-secondary-diagnoses-but-which-may-confound-clinical-assessment/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/are-fibromyalgia-and-depression-as-common-as-any-primary-diagnosis-in-routine-rheumatology-care-albeit-as-secondary-diagnoses-but-which-may-confound-clinical-assessment/