Session Information
Date: Tuesday, October 28, 2025
Title: (2377–2436) Systemic Lupus Erythematosus – Diagnosis, Manifestations, & Outcomes Poster III
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Systemic autoimmune rheumatic diseases (SARD) are a heterogeneous group of disorders marked by the presence of antinuclear antibodies (ANA), commonly detected by HEp-2 cell-based indirect immunofluorescence (IIF). The dense fine speckled (DFS) antinuclear antibody (ANA) pattern, caused by anti-DFS70 antibodies, is often misunderstood due to reported low association with SARD and presence in healthy individuals. Some studies suggest presence of isolated anti-DFS70 antibodies exclude SARD. Given the limited data from the Indian subcontinent and the large volume of ANA IIF tested, this study aims to estimate the prevalence and clinical associations of anti-DFS70 antibodies in sera tested for ANA without well defined disease, in nonrheumatic disease controls and in SARD patients.
Methods: Sera from SARD patients, those without a well-defined disease, and from non-rheumatic disease controls displaying a DFS IIF pattern, were further investigated using an anti-DFS70 ELISA and Line Immunoassay (LIA). ANA IIF was performed utilising HEp-20-10 based IIF.
Results: The DFS IIF pattern was observed in 82 out of 32,285 (0.25%) sera from referrals for undefined disease, 2 out of 350 (0.57%) in SARD sera and 1 out of 250 (0.4%) non-rheumatic disease controls. ELISA anti-DFS70 was positive in 74 of 82 ( 90%) undefined disease sera, 54 of 350 (15.4%) SARD sera and in 1 of 1 (100%) non-rheumatic disease control sera. Anti DFS70 LIA was positive in 74 of 82 ( 90%) undefined disease sera, 20 of 350 SARD sera(5.7%) and in 1 of 1 (100%) non-rheumatic disease control sera. There was almost perfect agreement (kappa value = 0.861) between anti-DFS70 ELISA and LIA in the routine ANA referral group. In SARD,anti-DFS70 ELISA positivity was significantly associated with higher prevalence of SLE (87% vs. 67.6%; p = 0.0033) and lower prevalence of RA (1.9% vs. 15.2%; p = 0.0040). Mean DFS ELISA titres in SLE patients with LIA positivity (n=14) were higher (3.38±1.61) compared to those negative for anti-DFS70 antibodies in LIA (1.55±0.63).SLE patients with positive anti-dsdna were significantly more likely to be anti-DFS70 ELISA positive (p=0.0001).SLE patients who tested positive for anti-DFS70 by ELISA had significantly higher disease activity, with a median SLE Disease Activity Index (SLEDAI) score of 16 (range: 10–23), compared to 10 (range: 5–15) in ELISA-negative patients (p = 0.01)Renal involvement significantly correlated with anti-DFS70 positivity in SLE patients; p=0.014.Monospecific anti-DFS70 antibodies in LIA were observed only in UCTD (3/4;75%), and none of the other SARD patients
Conclusion: When the DFS-IIF pattern is seen in sera with monospecific anti-DFS antibodies ( as tested in line immunoassay), SARD is less likely. Significant concordance between ELISA and Line immunoassay is noted for detecting anti-DFS70 antibodies. Anti-DFS70 antibodies, when present in SARD , coexist with other disease-associated antibodies and hence do not produce DFS IIF pattern. In SARD patients, anti-DFS70 ELISA positivity was significantly associated with SLE, higher disease activity (SLEDAI), anti-dsdna positivity, and renal involvement, while being inversely associated with RA.
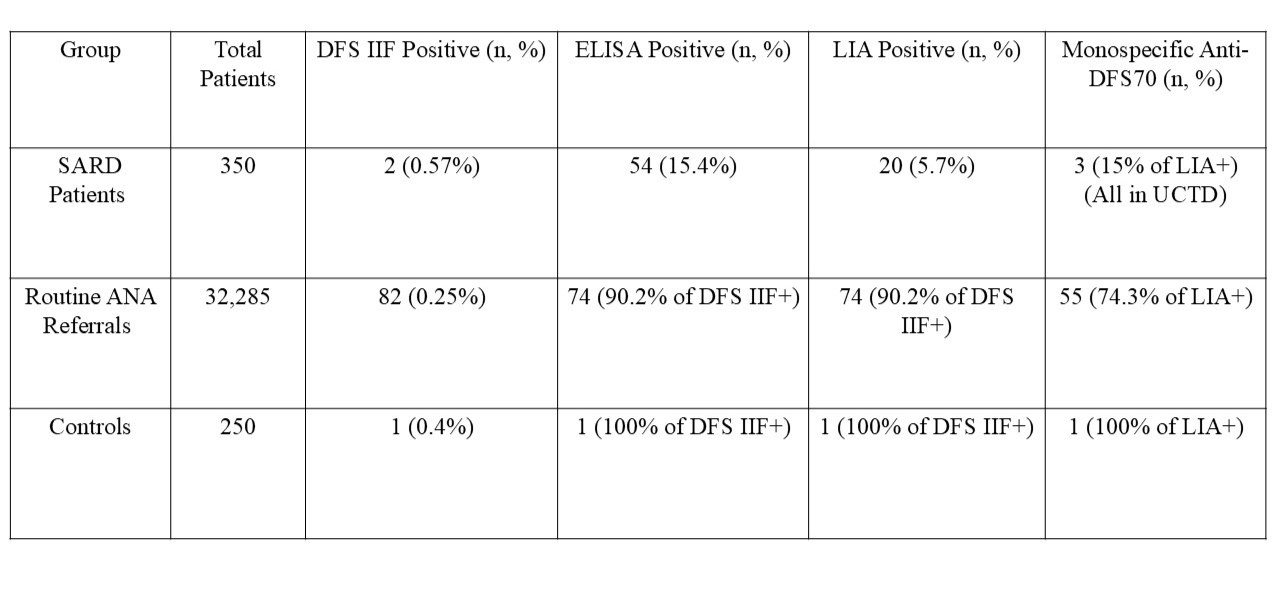 Table 1: Comparison of DFS IIF, Anti-DFS70 ELISA, LIA, and Monospecific Results
Table 1: Comparison of DFS IIF, Anti-DFS70 ELISA, LIA, and Monospecific Results
Across Study Groups
.jpg) Table 2: Demographic and Clinical Characteristics – (SARD Group)
Table 2: Demographic and Clinical Characteristics – (SARD Group)
.jpg) Table 3: Distribution of anti-DFS70 positivity by ELISA and LIA in various SARD
Table 3: Distribution of anti-DFS70 positivity by ELISA and LIA in various SARD
(n=54)
To cite this abstract in AMA style:
Mylavarapu R, Gavali M, Kashyap Parijeya B, Puranam K, rajasekhar L. Anti-dense fine speckled 70 antibodies in undefined disease, systemic autoimmune rheumatic diseases and controls [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/anti-dense-fine-speckled-70-antibodies-in-undefined-disease-systemic-autoimmune-rheumatic-diseases-and-controls/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/anti-dense-fine-speckled-70-antibodies-in-undefined-disease-systemic-autoimmune-rheumatic-diseases-and-controls/