Session Information
Date: Monday, October 27, 2025
Title: (1306–1346) Rheumatoid Arthritis – Diagnosis, Manifestations, and Outcomes Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Changes in serum cholesterol loading capacity (CLC) on macrophages were linked to coronary plaque progression in rheumatoid arthritis (RA). Inflammation, LDL oxidation and autoantibodies influenced macrophage cholesterol loading and plaque burden directly and indirectly. Oxidized LDL formed complexes with beta-2-glycoprotein-1 (b2GPI)—an antiatherogenic protein in serum and plaque—in both RA and controls. Complexes can be then bound by anti-b2GPI antibodies. Anti-b2GPI Ab, particularly of the IgA isotype, independently promoted coronary plaque progression in RA; yet the precise mechanisms remain speculative. We hypothesized that anti-b2GPI IgA may promote atherosclerosis progression by influencing oxidized LDL-mediated cholesterol loading on arterial macrophages.
Methods: Coronary CT angiography evaluated atherosclerosis (noncalcified, mixed, or calcified plaques) in 100 patients without cardiovascular disease at baseline and follow-up 6.9±0.4 years later. Presence of 5 plaques and lesions rendering greater than 50% stenosis were deemed extensive and obstructive disease respectively. CLC was measured as intracellular cholesterol content in serum treated human THP-1 monocyte-derived macrophages with a fluorimetric assay. Serum anti-b2GPI IgA were measured with ELISA at baseline and positivity was confirmed 12 weeks later. Negative binomial regression and logistic regression evaluated the influence of anti-b2GPI IgA on the relationship between CLC change and number of new plaques and likelihood of noncalcified plaque formation and new extensive or obstructive disease respectively.
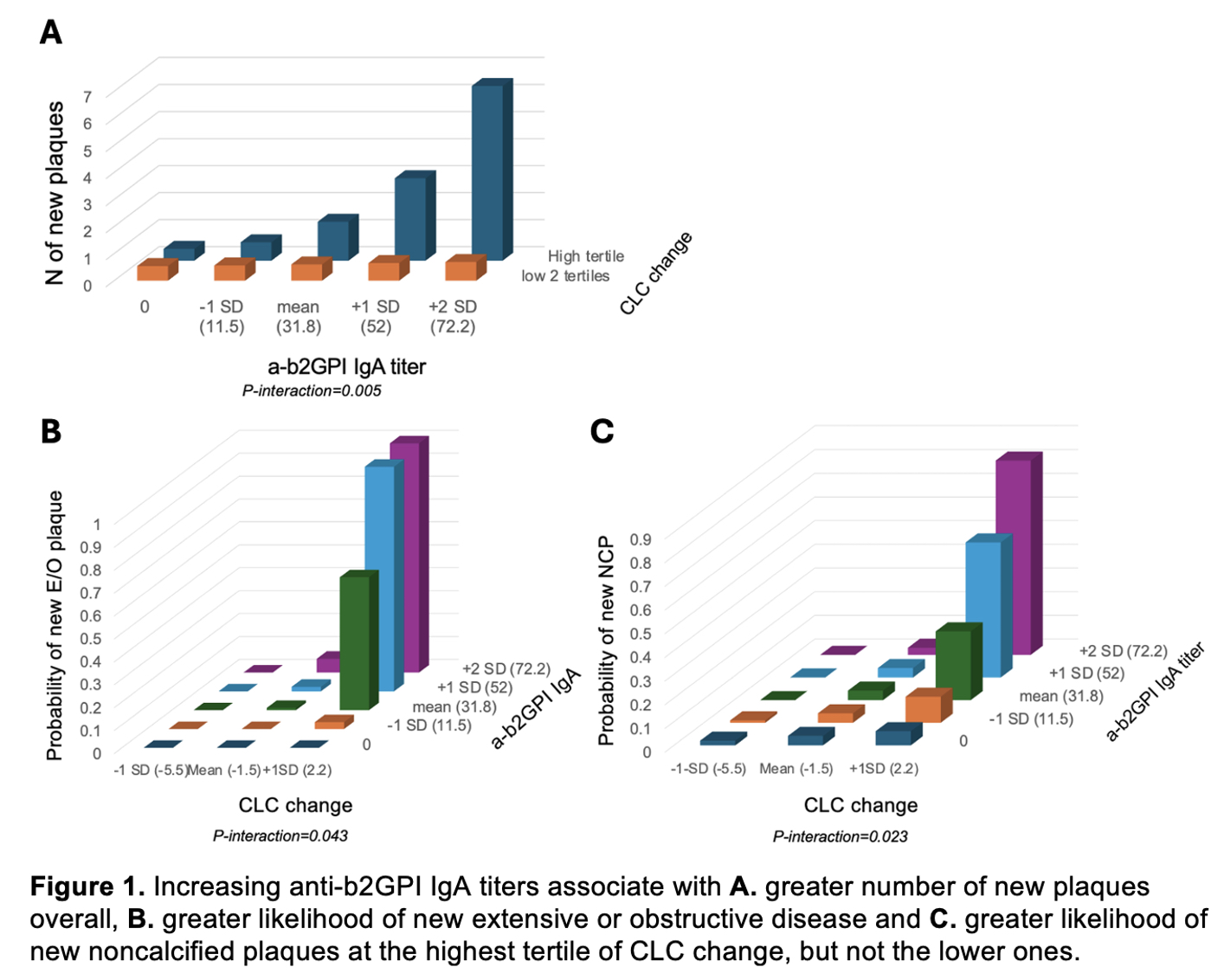
Results: A significant interaction between CLC change and anti-b2GPI IgA titers on plaque progression was observed. Specifically, increasing anti-b2GPI IgA titers associated with more new plaques overall (p for interaction=0.005), higher likelihood of new noncalcified plaque formation (p for interaction=0.023) and new extensive or obstructive disease (p for interaction=0.043) only at the highest tertile of CLC change (Figure 1). This suggested that anti-b2GPI IgA may be involved in macrophage cholesterol loading by oxidized LDL in a dose-dependent manner. Anti-b2GPI IgA may also determine the composition of newly formed plaques in the context of increasing CLC change (Figure 2). CLC change associated with a greater likelihood of higher-risk noncalcified plaque progression in the presence (odds ratio 2.82, 95% confidence interval 1.40-5.67) but not absence of anti-b2GPI IgA (p for interaction=0.005). In contrast, CLC change associated with a greater likelihood of lower-risk calcified plaque progression in the absence (odds ratio 1.48, 95% confidence interval 1.19-1.84) but not presence of anti-b2GPI IgA (p for interaction=0.046).
Conclusion: Anti-b2GPI IgA may facilitate macrophage cholesterol loading and influence coronary plaque progression and composition in a dose dependent manner, specifically at high levels of CLC change. Anti-b2GPI IgA may bind oxidized LDL/b2GP1 complexes to FcA receptors on arterial macrophages, promote cholesterol loading and atherosclerosis progression.
.jpg)
To cite this abstract in AMA style:
Karpouzas G, Papotti B, Ormseth S, Palumbo M, Budoff M, Ronda N. Anti-beta-2-glycoprotein-1 IgA antibodies facilitate macrophage cholesterol loading and influence coronary atherosclerosis progression in a dose-dependent manner in rheumatoid arthritis [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/anti-beta-2-glycoprotein-1-iga-antibodies-facilitate-macrophage-cholesterol-loading-and-influence-coronary-atherosclerosis-progression-in-a-dose-dependent-manner-in-rheumatoid-arthritis/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/anti-beta-2-glycoprotein-1-iga-antibodies-facilitate-macrophage-cholesterol-loading-and-influence-coronary-atherosclerosis-progression-in-a-dose-dependent-manner-in-rheumatoid-arthritis/