Session Information
Session Type: Abstract Session
Session Time: 1:00PM-2:30PM
Background/Purpose: Child opportunity is defined as the neighborhood resources and conditions that promote healthy childhood development. We determined whether low neighborhood-level opportunity associates with more severe disease presentation or higher acute care utilization after diagnosis in a geographically and socioeconomically diverse, multi-center cohort of patients with childhood-onset systemic lupus erythematosus (cSLE).
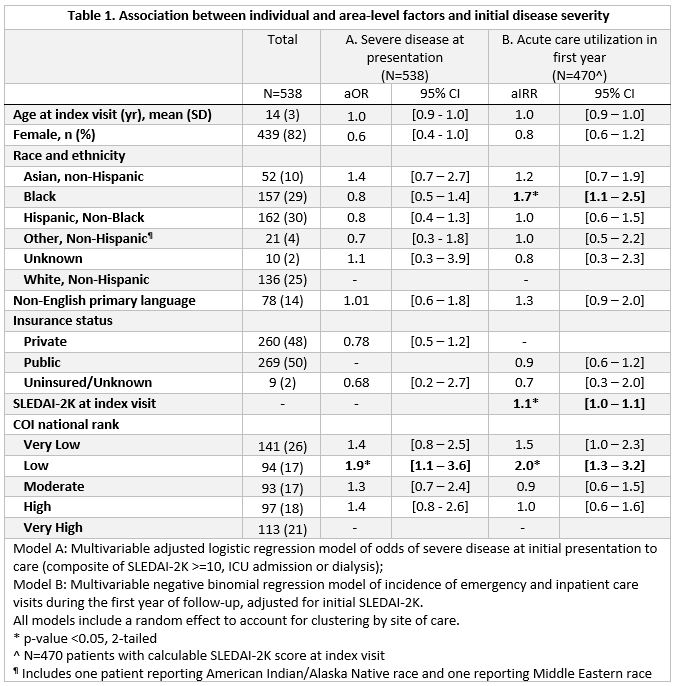
Methods: We identified patients with cSLE at 3 tertiary centers (Boston Children’s Hospital (BCH), Lurie Children’s Hospital of Chicago (LCH), and Children’s Hospital of Alabama (COA), 2016-2022) with valid U.S. street addresses and linked their medical records to census tract-level data. The index visit was the first visit with a physician diagnosis of SLE. The primary outcomes were severe initial disease presentation (composite of Systemic Lupus Erythematosus Disease Activity Index (SLEDAI-2K) ≥10, intensive care admission, or dialysis) and acute care utilization (inpateient or emergency visits) within the first year after the index visit. The secondary outcome was concurrent achievement of SLEDAI-2K < =4 and prednisone-equivalent dose < =7.5 mg/day at the most recent follow-up visit. The exposure of interest was census tract-level Child Opportunity Index (COI) 2.0 (29 indicators across education, socioeconomic status, physical environment), ranked nationally. Associations between COI and outcomes were estimated using logistic or negative binomial regression accounting for clustering by site. Patient-level covariates included age at SLE onset, sex, race and ethnicity reported in the medical record, English vs. non-English primary language and insurance status.
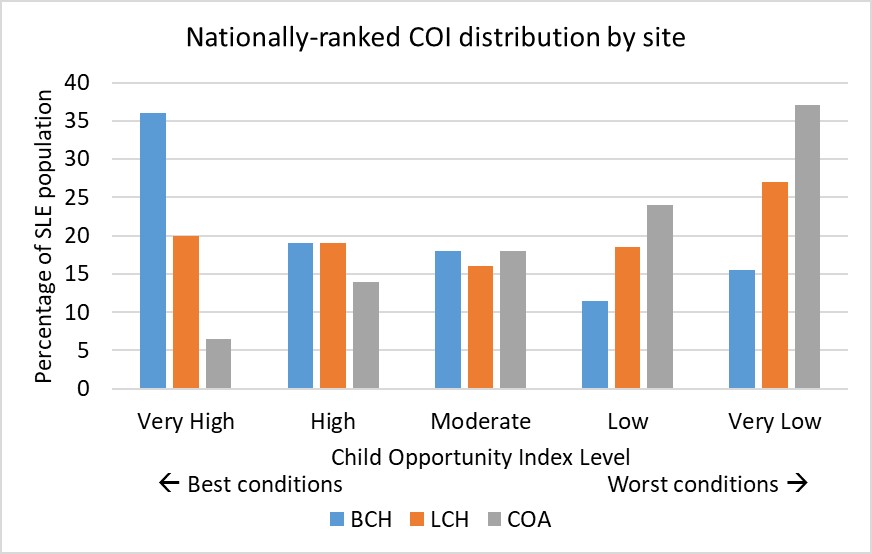
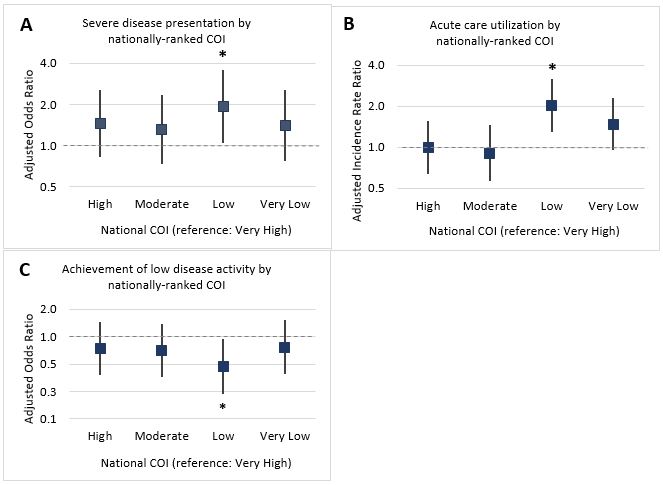
Results: We included 148 patients with cSLE at BCH, 265 at LCH, and 138 at COA. Of 538 patients with evaluable COI linkages, 50% were publicly insured, 29% reported Black race, 30% reported Hispanic ethnicity, and 14% had a preferred language other than English (Table 1). COA had the highest proportion of Black patients (59%) while LCH had the highest proportion of Hispanic patients (43%). COI was on average higher at BCH compared to LCH and COA (Fig. 1). 50% of cSLE patients met criteria for severe presentation, and the median number of inpatient/emergency visits in the 1st year was 1 [range 1-13]. Living in areas with low vs. very high COI associated with 1.93 higher adjusted odds of severe presentation (95% CI [1.05-3.57]; Fig. 2A), 2.03 higher adjusted incidence of acute care utilization during the first year of follow-up (95% CI [1.29-3.18]; Fig. 2B and Table 1), and 0.47 lower odds of achieving SLEDAI-2K < =4 and prednisone < =7.5 mg/day adjusted for severe disease presentation (95% CI [0.23–0.94]; Fig. 2C).
Conclusion: Higher cSLE disease severity at presentation to care and lower likelihood of achieving disease targets after establishing subspecialty care were associated with living in areas with lower child opportunity, which may represent structural barriers to care and effects of toxic stress, among other socio-environmental factors. Tailoring community-based interventions to neighborhoods with low levels of child opportunity may reduce disparities at multiple points of access to pediatric subspecialty care.
To cite this abstract in AMA style:
Chang J, Liu J, Smitherman E, Patel P, Alonzi G, Morgan G, Timmerman L, Berbert L, Weller E, Costenbader K, Son M. A Multi-center Study of Associations Between Neighborhood-Level Child Opportunity, Initial Disease Severity and Acute Care Utilization Among Children with SLE [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/a-multi-center-study-of-associations-between-neighborhood-level-child-opportunity-initial-disease-severity-and-acute-care-utilization-among-children-with-sle/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/a-multi-center-study-of-associations-between-neighborhood-level-child-opportunity-initial-disease-severity-and-acute-care-utilization-among-children-with-sle/