Session Information
Date: Tuesday, October 28, 2025
Title: (2106–2123) Osteoporosis & Metabolic Bone Disease – Basic & Clinical Science Poster II
Session Type: Poster Session C
Session Time: 10:30AM-12:30PM
Background/Purpose: Osteoporosis, sarcopenia, and frailty are the 3 determinants of aging. A novel syndrome of combined osteosarcopenia has negative health outcomes among geriatric populations. In the last decades, studies have been conducted to assess sclerostin role in the bone and muscle cross-talk. Sclerostin is a protein produced by osteocytes, but recently it has been proposed to be secreted from myocytes as well. This study aimed to assess the level of serum sclerostin in osteoporosis, sarcopenia, and osteosarcopenia to address its possible dual role on bone and muscle units.
Methods: This cross-sectional study included 66 females aged ≥ 60 years old equally divided into 3 groups: “osteoporosis”, “sarcopenia” and “osteosarcopenia” as follows: (a) females with osteoporosis were assessed by dual-energy X-ray absorptiometry (DXA) scan at the hip, lumbar spine, or distal 1/3 of the radius with a T-score ≤ -2.5 standard deviation (SD). (b) Females with sarcopenia were diagnosed according to the 2018 revised criteria of the European Working Group on Sarcopenia in Older People (EWGSOP). (c) Females with osteoporosis or osteopenia (T-score -1 to < -2.5) and sarcopenia were in osteosarcopenia group. Fracture risk assessment score (FRAX) was done using an online FRAX calculator according to our geographic region. Anthropometric measurements and comprehensive geriatric assessment, including frailty, nutritional, functional assessment, and serum sclerostin level, were done for all subjects.
Results: We determined the optimum cut-off value of sclerostin in differentiating between each 2 groups. Results were adjusted for age and BMI. Serum sclerostin showed the highest level in the osteoporosis group with a cutoff level ≥ 1.29 ng/ml (sensitivity 66.7%, specificity 68.2%). The lowest level was among the sarcopenia group with a cutoff level < 0.7 ng/ml (sensitivity 75%, specificity of 59.1%). In osteosarcopenia, we found that sclerostin level was ≥ 0.7 ng/ml and < 1.29 ng/ml (sensitivity of 66.7%, specificity of 68.2%). Osteosarcopenia group had the least serum albumin, body mass index (BMI), muscle mass, bone mineral density (BMD), and android/gynecoid (A/G) ratio. They had the most advanced age, the highest fracture risk (FRAX) score of major osteoporotic and hip fractures. They had the worst nutritional state and the most functional impairment.
Conclusion: Sclerostin could have an anabolic effect on muscles and a catabolic effect on bone. Advanced age, low serum albumin, low body weight, and poor nutritional state are highest in osteosarcopenia. Osteosarcopenia patients are at higher risk for developing future fractures.
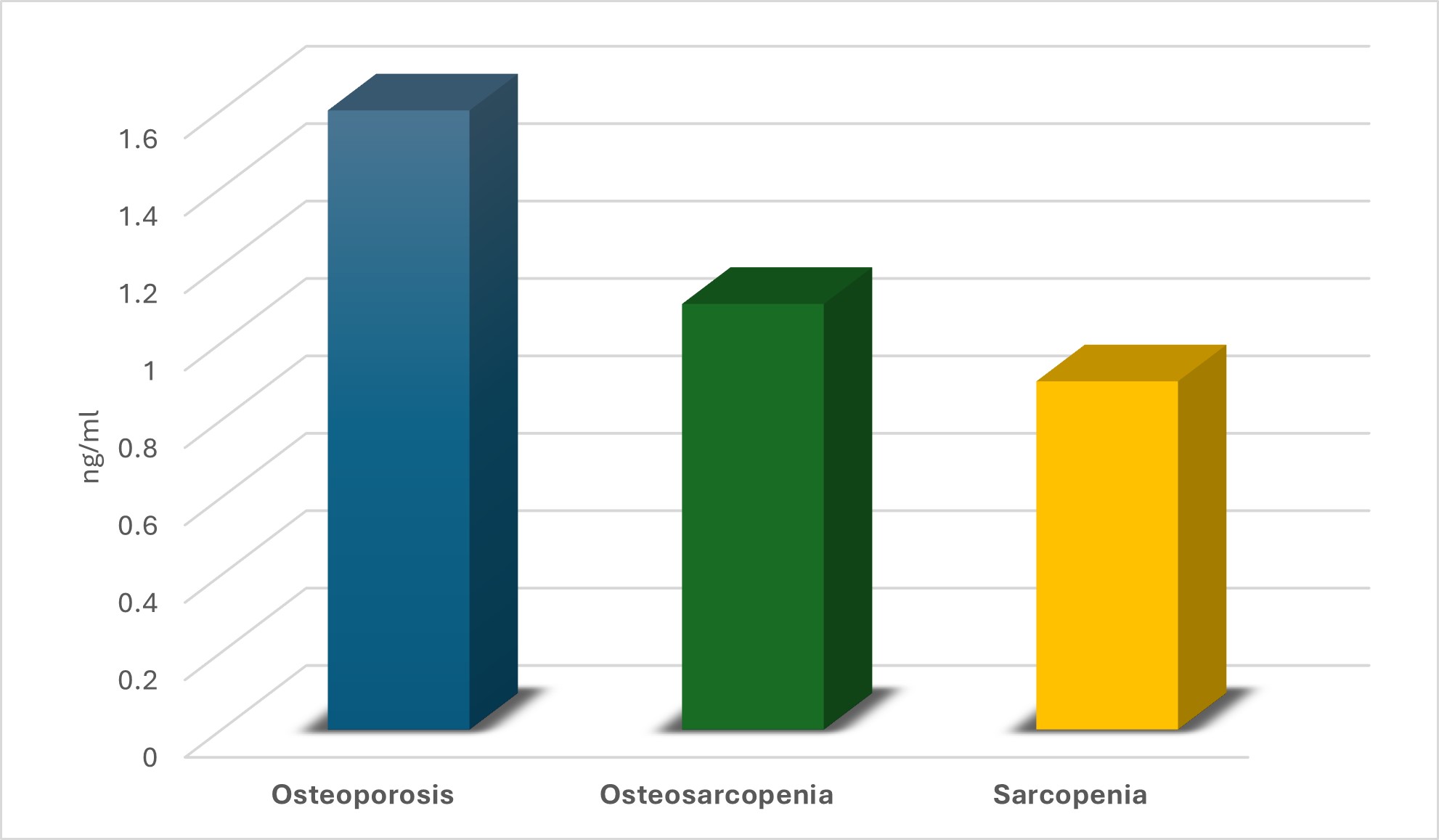 Figure 1: Mean sclerostin (ng/ml) in the 3 study groups
Figure 1: Mean sclerostin (ng/ml) in the 3 study groups
.jpg) Table 1: Summary of the group that had the highest and the lowest statistically significant mean values for each variable.
Table 1: Summary of the group that had the highest and the lowest statistically significant mean values for each variable.
To cite this abstract in AMA style:
Hegazy M, Fayed F, Mahgoub S, El Ebrashy Y, Hossam Al-Din Ibrahim M. Sclerostin in Aging Bone and Muscle: A Comparative Study of Osteoporosis, Sarcopenia, and Osteosarcopenia [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/sclerostin-in-aging-bone-and-muscle-a-comparative-study-of-osteoporosis-sarcopenia-and-osteosarcopenia/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/sclerostin-in-aging-bone-and-muscle-a-comparative-study-of-osteoporosis-sarcopenia-and-osteosarcopenia/