Session Information
Date: Monday, October 27, 2025
Title: (1191–1220) Muscle Biology, Myositis & Myopathies – Basic & Clinical Science Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Idiopathic inflammatory myopathies (IIM) are a group of rare and heterogeneous diseases. One of the greatest challenges in IIM management is defining and predicting disease flares, which are inconsistently characterized across studies(1–2). The aim of the study was to identify predictors of relapse in a retro-prospective, multicenter IIM cohort during the first two years of disease.
Methods: Patients with IIM subsets—dermatomyositis (DM), polymyositis (PM), antisynthetase syndrome (ASyS), connective tissue disease-associated IIM (CTD-IIM), or immune-mediated necrotizing myopathy (IMNM)—were included if aged ≥18 years and had ≥2 years of follow-up. Relapse was defined as any worsening of disease activity requiring escalation of immunosuppressive therapy and/or glucocorticords (GC). Patients were classified as monophasic (M; 0 relapses), polycyclic (P; ≥1 relapse), or chronic continuous (CC; persistent activity) (2). Clinical characteristics across subgroups were compared using chi-square, Mann–Whitney U, or Student’s t-test. Predictors were identified through multivariable logistic regression.
Results: Of 297 screened patients, 206 were included (155 F; median age at diagnosis: 46.9 years), distributed as follows: DM (82; 39.8%), ASyS (56; 27.2%), CTD-IIM (40; 19.4%), PM (14; 6.8%) and IMNM (14; 6.8%).Over the first 2 years, disease trajectories were M in 40.8% of patients (n=84), P in 32.5% (n=67) and CC in the remaining (n=55, 26.7%). PM and IMNM demonstrated a higher propensity for CC or P patterns (64.2% vs 35.8%, p=0.326) although autoantibodies were not predictive.Among 139 documented relapses, muscle involvement predominated (61.9%), with subtype-specific patterns: PM/IMNM (88.9% muscle), DM (68.4% muscle and skin), and ASyS (61.4% ILD). Refractory disease was primarily associated with relapse (43.2%), followed by treatment-related factors (see Figure 2B). Most relapses (56.5%) occurred while patients were on low-dose GC (≤5mg/day or none) with 44.7% developing within 6 months of stable dosing. Relapses occurred equally during short-term (≤3 months) and long-term ( >1 year) stable immunosuppressive therapy (30.2% each).P/CC disease was associated with a more severe phenotype— including elevated muscle enzymes and higher global assessment scores (Ph and Pt). Patients with relapsing patterns more often received low-dose GC at disease onset ( < 0.25 mg/kg; 78.9% vs 21.1%, p=0.019) and intravenous immunoglobulin therapy (26.0% vs 10.0%, p=0.004). Multivariable analysis confirmed baseline muscle involvement, CPK levels, and PtGA as independent predictors of relapse.
Conclusion: In this multicentric cohort, relapses occurred in two-thirds of patients, often during a vulnerable period on low-dose GC and within six months of stable therapy. High baseline CPK and PtGA, along with low initial GC dose, independently predicted relapse. These findings highlight the potential value of flare predictors and advocate for standardized definitions of disease activity/relapse in IIM.ReferencesAggarwal R, et al. ACR/EULAR response criteria for DM/PM. Ann Rheum Dis. 2017;76(5):792–801.Constantin T, et al. Relapse and survival in juvenile/adult DM. Orv Hetil. 2007;148(42):1989–97.
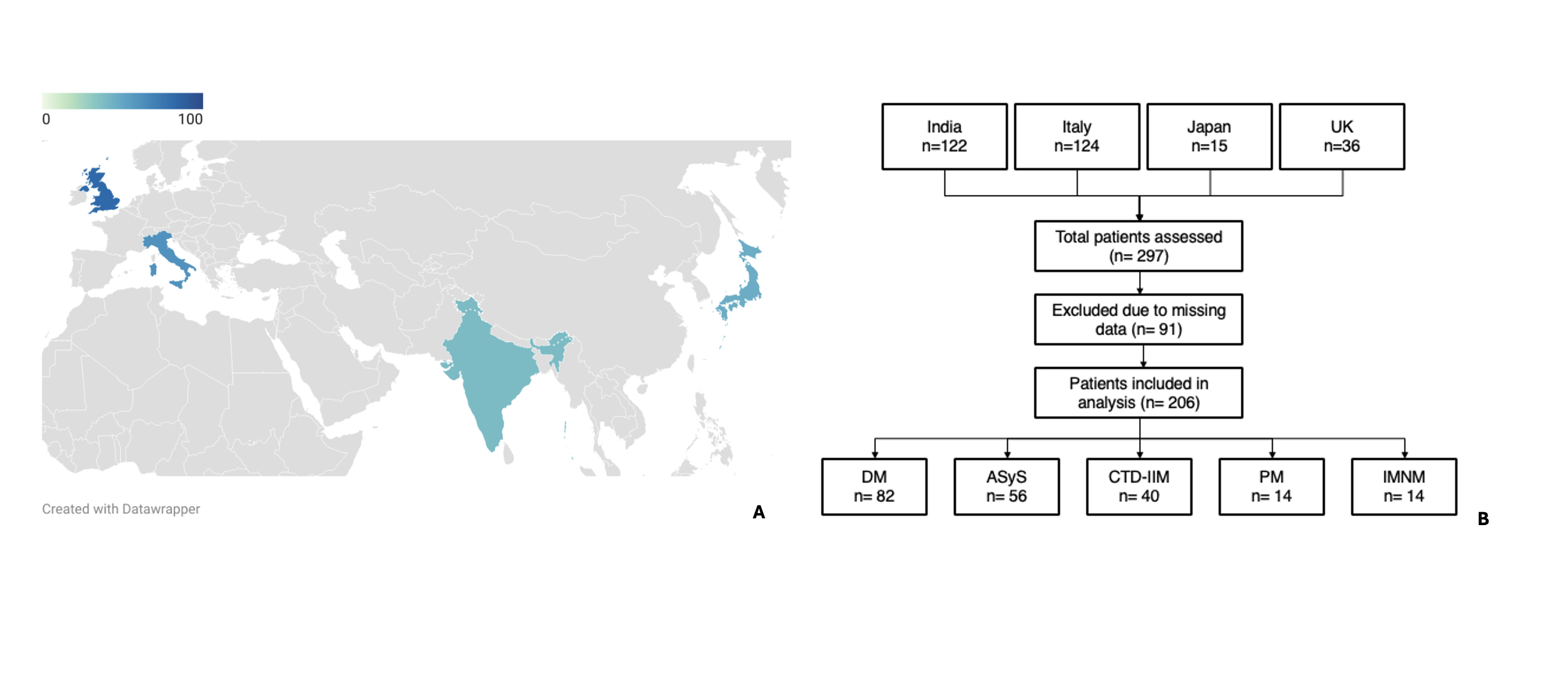 Figure 1A: Percentage of non-monophasic patients in participating centers. 1B: Workflow chart of patients’ selection
Figure 1A: Percentage of non-monophasic patients in participating centers. 1B: Workflow chart of patients’ selection
.jpg) Figure 2A: Clinical predictors of chronic/relapsing disease in IIM. 2B Causes of relapses in different IIM subsets
Figure 2A: Clinical predictors of chronic/relapsing disease in IIM. 2B Causes of relapses in different IIM subsets
.jpg) Table 1. Characteristics of monophasic versus non monophasic patients.
Table 1. Characteristics of monophasic versus non monophasic patients.
To cite this abstract in AMA style:
Pellico M, Bochicchio C, Iannone C, Minikumari Rahulan L, Fornaro M, Cavazzana I, Conticini E, Kuwana M, Yoshida A, Cavalli S, Grazzini S, Gatti A, Lopinto G, Semeraro P, Sheeran T, Iannone F, Agarwal V, Caporali R, Del pAPA N, Gupta L. Relapse in Idiopathic Inflammatory Myopathies: insights from extended MyoCite and Italian Consortia [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/relapse-in-idiopathic-inflammatory-myopathies-insights-from-extended-myocite-and-italian-consortia/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/relapse-in-idiopathic-inflammatory-myopathies-insights-from-extended-myocite-and-italian-consortia/