Session Information
Date: Monday, October 27, 2025
Title: (1147–1190) Miscellaneous Rheumatic & Inflammatory Diseases Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Recurrent pericarditis (RP) is a chronic autoinflammatory disease mediated by IL-1 that requires long-term treatment. While the 2015 European Society of Cardiology Guidelines position IL-1 pathway inhibition only after corticosteroids, complications associated with long-term steroid use underscore the importance of steroid-sparing strategies. Rilonacept, an IL-1a and IL-1b cytokine trap, is the only FDA-approved treatment for RP (available since April 2021). RESONANCE, an ongoing 5-year non-interventional US registry of patients (pts) with RP, has collected real-world data from pts cared for by cardiologists with a focus on pericardial disease, with a goal of informing contemporary RP clinical management.
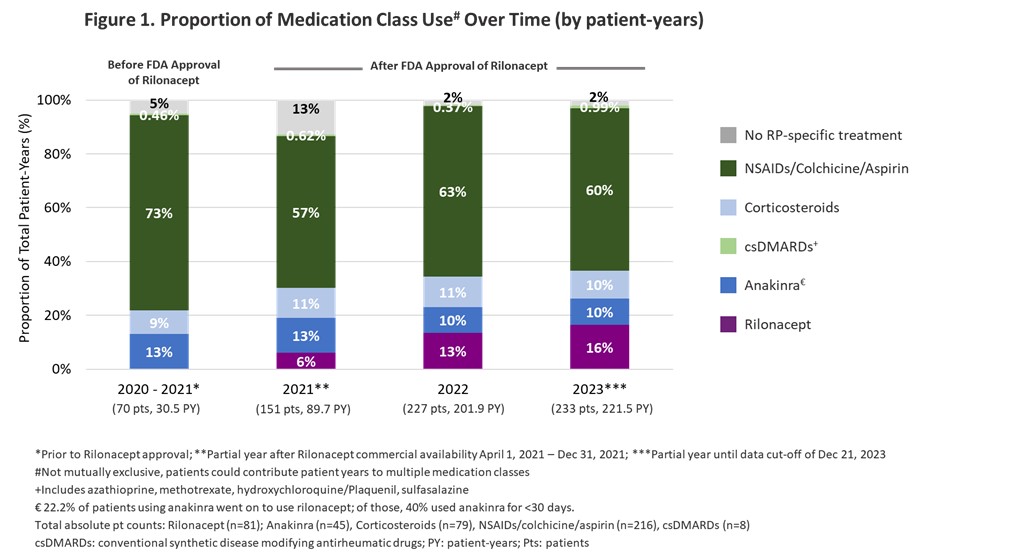
Methods: From a database cut-off (DCO) on 21 December 2023, patient demographics and disease characteristics are reported for 242 active RP pts (excluding RHAPSODY prior participants) at 20 US sites (median [Q1:Q3] 2.1 [1.5:2.6] years and 556 patient-years [PY] of observation). Complete medication class use data were available for 239 pts (total 546 PY). Proportional medication class use prior to initiating rilonacept was analyzed annually across the observation period.
Results: Mean (standard deviation) age at DCO was 50.2 (16.6) years; 58.1% were female. Median [Q1:Q3] disease duration at DCO from index pericarditis episode was 3.1 [2.2:5] years. Median [Q1:Q3] number of prior recurrences at enrollment was 3 [2:5]. Prior to rilonacept availability, NSAIDs/Colchicine/Aspirin represented the highest proportion of treatment (73% of PY); steroid use was 9% of PY, IL-1 pathway inhibition (anakinra) was 13% of PY, and conventional synthetic disease modifying antirheumatic drugs (csDMARDs) were 0.46% PY (no RP-specific treatment was 5% of PY) (Fig 1). In the years since rilonacept availability, proportional IL-1 pathway inhibition use has increased, from 13% of PY in 2020-21 to 26% of PY in 2023, driven by an increase in rilonacept use (6%, 13%, 16% of PY in 2021, 2022, and 2023, respectively). Over that same period, proportional NSAIDs/Colchicine/Aspirin use (57%-63% of PY) has been consistently 6-times more than proportional steroid use (10%-11% of PY). Among pts who initiated rilonacept (n=81), similar proportions transitioned from NSAIDs/Colchicine/Aspirin as from corticosteroids (Fig 2), a robust trend observed each year. Of those pts transitioning from corticosteroids, 1/3 had used corticosteroids for < 30 days and 1/3 for >6 months.
Conclusion: Real-world data from the RESONANCE registry reveal a temporal shift in RP management in US centers with RP-focused cardiologists, with increased proportional IL-1 pathway inhibition use since rilonacept availability in 2021. Advancing beyond 2015 guideline recommendations, IL-1 pathway inhibition is often being used as steroid-sparing treatment, i.e., after colchicine instead of chronic corticosteroids.
.jpg)
To cite this abstract in AMA style:
Cremer P, Garshick M, Luis S, Raisinghani A, Weber B, Parameswaran V, Curtis A, Gibbons S, Klein A, Paolini J. Increased Adoption of IL-1 Pathway Inhibition and the Steroid-sparing Paradigm Shift: Temporal Trends in Recurrent Pericarditis Treatment From the RESONANCE Patient Registry [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/increased-adoption-of-il-1-pathway-inhibition-and-the-steroid-sparing-paradigm-shift-temporal-trends-in-recurrent-pericarditis-treatment-from-the-resonance-patient-registry/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/increased-adoption-of-il-1-pathway-inhibition-and-the-steroid-sparing-paradigm-shift-temporal-trends-in-recurrent-pericarditis-treatment-from-the-resonance-patient-registry/