Session Information
Date: Monday, October 27, 2025
Title: (1147–1190) Miscellaneous Rheumatic & Inflammatory Diseases Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Sarcoidosis is an inflammatory disease characterized by non-necrotizing granulomatous inflammation that can affect any organ. Approximately 5% of patients with sarcoidosis develop clinically significant cardiac sarcoidosis (CS), but up to one-fourth may have clinically silent cardiac involvement. A definitive diagnosis of CS requires histologic evidence of granulomas in cardiac tissue. Due to the limited sensitivity and infrequent use of cardiac biopsies, the pursuit of a tissue diagnosis is not routinely performed. There is a paucity of data on biopsy-confirmed CS, particularly among Black patients, a population at higher risk for this disease. We aimed to characterize a cohort of Black patients with biopsy-proven CS and describe their clinical features and outcomes.
Methods: We conducted a retrospective study via review of electronic medical records. Patients with CS in our institution’s cardiac sarcoidosis database (2014 – 2025) were identified. Black patients with biopsy-proven CS (referred to as definite CS as per the Heart Rhythm Society criteria) were included in our study. We assessed demographic, clinical presentation, diagnostic evaluation, immunosuppression, heart replacement therapies, and outcomes.
Results: Amongst 306 definite or probable CS patients, 17 Black patients had definite CS. The diagnosis was established through histopathology from endomyocardial biopsy (n = 12) or explanted heart tissue (n = 5). Demographic and clinical characteristics are summarized in Table 1. Most patients (94%) had heart failure with reduced ejection fraction, with 71% having severe left ventricular systolic dysfunction (ejection fraction < 30%). In 53% of the patients, CS was the first diagnosis of sarcoidosis. Isolated cardiac sarcoidosis was diagnosed in 18% of the patients. Almost 60% had increased multifocal uptake on PET scans at diagnosis. The median initial dose of prednisone was 40 mg (range: 20–80 mg), and the median duration of treatment was 1 year (range: 0–11 years). Mycophenolate was the most frequently used (41%) steroid-sparing agent for immunosuppression, followed by methotrexate (24%). Adalimumab and infliximab were used as second-line steroid-sparing agents (18%). Seven patients ultimately received heart transplants. Post-transplant immunosuppression typically included prednisone, mycophenolate, and tacrolimus. Over a median duration of seven years, five patients died (three of these had not received any maintenance immunosuppression), one was lost to follow-up, and the rest were clinically stable or in remission. There was no recurrence of CS in any of the patients who received heart transplantation.
Conclusion: To our knowledge, this is the largest descriptive cohort of biopsy-proven CS in Black patients. One-third of the patients in our study were diagnosed with CS after heart transplantation, which highlights the challenge in making a definitive diagnosis. Given the rarity of definite CS, multi-institutional registry study would be useful to characterize disease presentation and diagnosis.
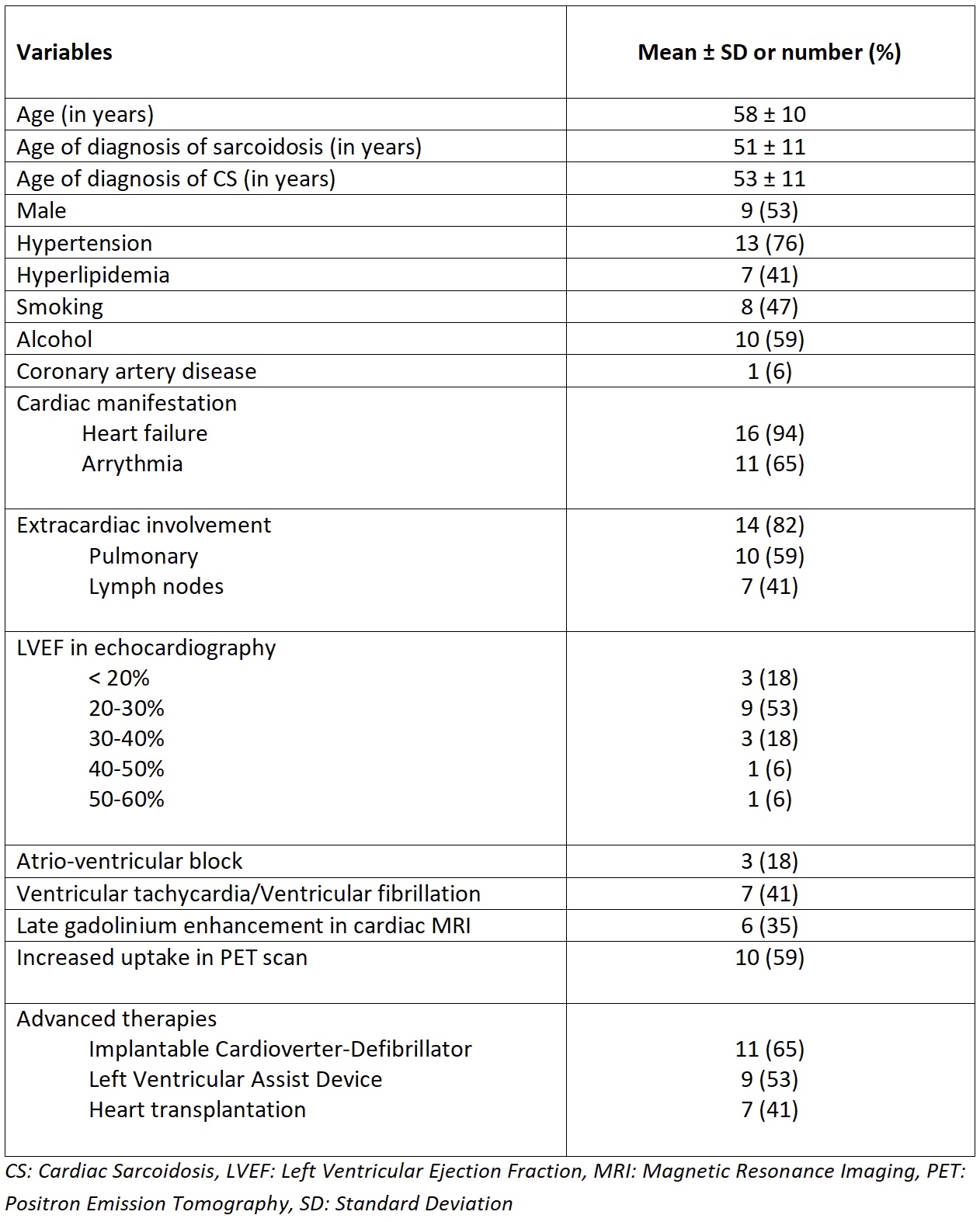 Table 1: Characteristics of the definite cardiac sarcoidosis in Black patients
Table 1: Characteristics of the definite cardiac sarcoidosis in Black patients
To cite this abstract in AMA style:
Subedi R, Haddad H, Barish R, Vora T, Afari-Armah N, Kadakkal A, Sheikh F, Constantinescu F. Cardiac Sarcoidosis in Black Patients: A Biopsy-Confirmed Cohort Study [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/cardiac-sarcoidosis-in-black-patients-a-biopsy-confirmed-cohort-study/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/cardiac-sarcoidosis-in-black-patients-a-biopsy-confirmed-cohort-study/