Session Information
Date: Monday, October 27, 2025
Title: (1147–1190) Miscellaneous Rheumatic & Inflammatory Diseases Poster II
Session Type: Poster Session B
Session Time: 10:30AM-12:30PM
Background/Purpose: Sarcoidosis is a systemic autoimmune disease with multiorgan involvement. In this study, we analyzed the differences in characteristics in patients with sarcoid myocarditis (cardiac sarcoidosis) and sarcoidosis with other systemic manifestations (other sarcoidosis).
Methods: A retrospective cohort study was performed using TriNetX, a global federated health research network that provides access to electronic medical records across large health care organizations (HCOs). Data was used from 102 HCOs. Patients (>18 years old) were divided into two cohorts, based on the presence of cardiac sarcoidosis (ICD-10 D86.8) or other systemic manifestations of sarcoidosis. 1:1 propensity score matching was performed using 27 different baseline characteristics (Table 1 and Table 2). Kaplan-Meier survival analysis was performed to look at differences in mortality.
Results: 10,296 patients were included in the cardiac sarcoidosis cohort and 160,918 patients were included in the other sarcoidosis cohort before propensity score matching. After propensity score matching, 10,046 patients were included in each cohort. Univariate analysis before matching showed several significant differences (Table 1 and Table 2). After propensity score matching, there was a significantly higher frequency of black or African American patients with cardiac sarcoidosis (p=0.003), where other sarcoidosis had a significantly higher frequency of white patients (p < 0.001, Table 1). Patients with cardiac sarcoidosis had a significantly increased frequency of hypertension (p=0.007), lung, cutaneous, and lymph node involvement (p< 0.001) and significantly higher frequencies of meningitis (p=0.016), iridocyclitis, arthropathy, and myositis (p< 0.001) (Table 1). The frequency of elevated ESR, CRP, and medication usage was not significantly different (Table 2). Mortality risk was 10.1% in the cardiac sarcoidosis group vs. 15.8% in the other sarcoidosis group, resulting in a statistically significant risk difference of –5.7%, indicating a lower absolute risk of death in the myocarditis group (Figure 1A). Risk ratio was 0.64 (95% CI: 0.60–0.69) and odds ratio was 0.60 (95% CI: 0.55–0.65), suggesting a ~40% reduction in the relative risk or odds of mortality in the cardiac sarcoidosis group (Figure 1A). Kaplan-Meier survival analysis also showed that the survival probability at the end of study period was higher in those with myocarditis (60.99%) than those without (50.33%) (Figure 1B). The difference was statistically significant (log-rank test χ² = 33.54, p < 0.001). Cox regression analysis yielded a hazard ratio of 0.79 (95% CI: 0.73–0.86, p = 0.002), indicating a 21% lower hazard of death over time in the myocarditis group, with the proportional hazards assumption met.
Conclusion: Black or African American race and several organ-specific sarcoidosis subtypes remained more prevalent in the cardiac sarcoidosis group after matching, suggesting that cardiac sarcoidosis may represent a distinct systemic phenotype with more frequent multiorgan involvement. Contrary to expectations, patients with sarcoid myocarditis demonstrated a lower mortality risk and better survival compared to sarcoidosis patients without myocarditis.
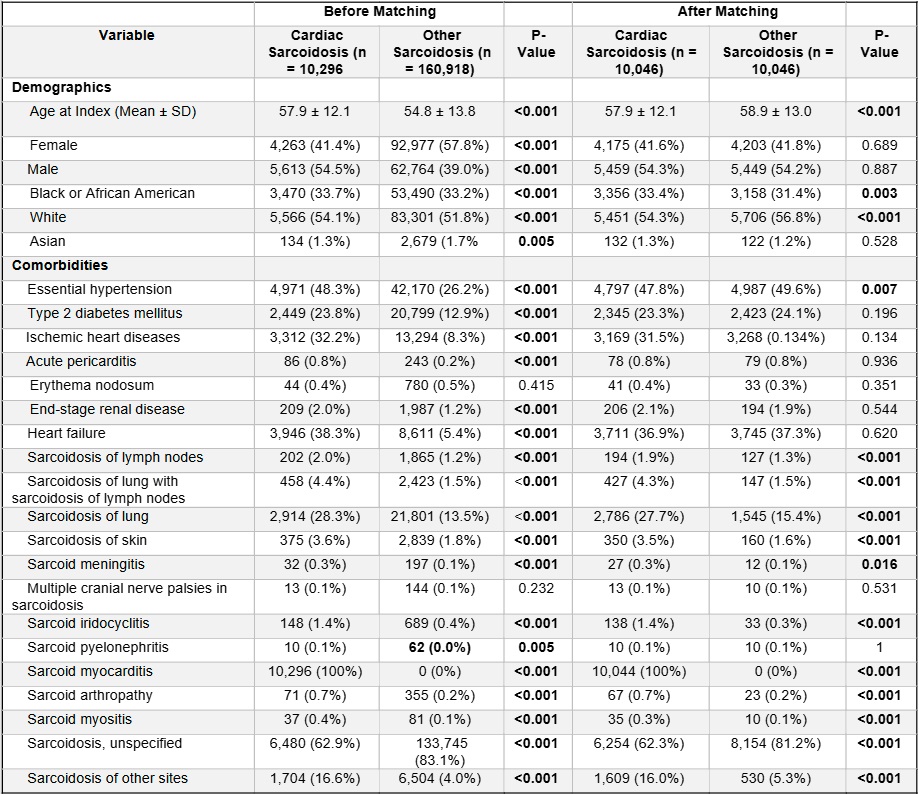 Table 1. Baseline Characteristics of Patients with Cardiac Sarcoidosis vs. Other Sarcoidosis
Table 1. Baseline Characteristics of Patients with Cardiac Sarcoidosis vs. Other Sarcoidosis
.jpg) Table 2. Serological Profiles and Medications Used in Patients with Cardiac Sarcoidosis vs. Other Sarcoidosis
Table 2. Serological Profiles and Medications Used in Patients with Cardiac Sarcoidosis vs. Other Sarcoidosis
.jpg) Figure 1A. Mortality Risk Analysis of Patients with Cardiac Sarcoidosis vs. Other Sarcoidosis
Figure 1A. Mortality Risk Analysis of Patients with Cardiac Sarcoidosis vs. Other Sarcoidosis
Figure 1B. Kaplan-Meier Survival Analysis of Mortality in Patients with Cardiac Sarcoidosis vs. Other Sarcoidosis
To cite this abstract in AMA style:
Guan C, Nachawati D, Daneshvar A, Pfeil K, Harper E, Frumker L, Gump M, Nahra V, Pamuk O. A Comparison of Patients with Cardiac Sarcoidosis vs. Other Systemic Manifestations of Sarcoidosis: A Retrospective Cohort Study [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/a-comparison-of-patients-with-cardiac-sarcoidosis-vs-other-systemic-manifestations-of-sarcoidosis-a-retrospective-cohort-study/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/a-comparison-of-patients-with-cardiac-sarcoidosis-vs-other-systemic-manifestations-of-sarcoidosis-a-retrospective-cohort-study/