Session Information
Date: Sunday, October 26, 2025
Title: (0593–0640) Systemic Lupus Erythematosus – Diagnosis, Manifestations, & Outcomes Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: HCQ induced cardiomyopathy leading to heart failure is a rare but serious potential treatment complication. Currently there are no screening guidelines for detecting HCQ related cardiotoxicity. This study aims to identify signs of cardiotoxicity, including cardiomyopathy, in patients on HCQ. Secondary objectives include identifying non-invasive modalities for detection of HCQ induced cardiac toxicity.
Methods: We conducted a cross-sectional observational study from 2023 to 2025 at an academic medical center. We included patients aged 18–75 with a confirmed diagnosis of rheumatic disease and current HCQ therapy. We excluded patients with known history of cardiomyopathy from an alternative etiology. BNP, Troponin, serum HCQ level, ECG and echocardiogram were performed. Interventricular septal thickness at end-diastole (IVSd), an established echocardiogram criterion for LVH and a reported early finding of HCQ cardiac toxicity, was documented (1). Patients with increased IVsd ( >1.2cm) and/or other cardiac abnormalities were referred to cardiology for further evaluation and possible biopsy.
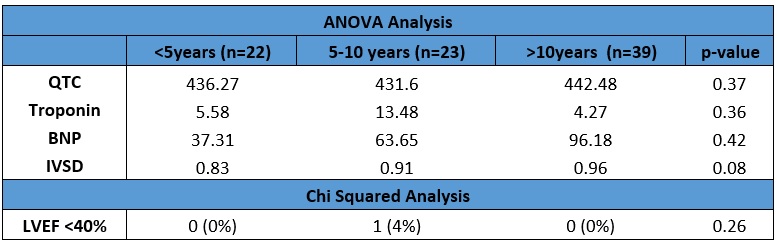
Results: We evaluated 84 patients on HCQ, with baseline characteristics summarized in Table 1. Patients were divided into three groups based on treatment duration and cardiac parameters were compared (Table 2). Cardiac abnormalities of QTc > 440 ms were observed in 25 patients, IVSd > 1.2 cm in 7 patients, BNP > 100 pg/mL in 18 patients, troponin elevation in one patient, and reduced EF ( < 40%) in one patient. Two patients underwent cardiac biopsy with findings consistent with HCQ toxicity. Both had MCTD diagnosis (SLE/SSc and positive anti-RNP), were on HCQ for over 10 years, had GFR < 40, QTc >450 ms; one had IVSd > 1.2 cm, and both had normal EF. ANOVA analysis did not show statistically significant differences in QTc, troponin, BNP or IVSd between the treatment duration groups. A chi-squared test assessing EF by HCQ duration also showed no significant difference (p = 0.24). A secondary analysis using a one-tailed t-test revealed a statistically significant difference in IVSd between patients receiving HCQ for >10 years compared to those treated for < 10 years (p = 0.03).
Conclusion: Our study found no statistically significant difference between the duration of HCQ use and measures of cardiac toxicity. Overall, abnormal cardiac findings were infrequent and did not correlate with HCQ exposure length. Numerically, there is a trend toward increased LVH in patients on long-term HCQ ( >10 years), and a secondary analysis shows a statistically significant difference in IVSd between patients on HCQ for >10 years compared to those treated for < 10 years. However, given the small sample size in this cross-sectional study, a definitive association cannot be established. IVSd appears to be superior to EF as a noninvasive marker for potential HCQ cardiac toxicity. Similar to HCQ retinal toxicity, patients with reduced GFR and higher cumulative dose may benefit from enhanced screening.1. Tselios K, Deeb M, Gladman DD, Harvey P, Urowitz MB. Antimalarial-induced cardiomyopathy: a systematic review of the literature. Lupus. 2018 Apr;27(4):591-599. doi: 10.1177/0961203317734922. Epub 2017 Oct 9. PMID: 28992800.
.jpg)
.jpg)
To cite this abstract in AMA style:
Bhatti J, Lee K, Sanghavi N, Zak S, Ash J, Miceli J, Sperber K, Pan S, Wasserman A. Study of Long Term HCQ Safety on Cardiac Muscle Function in Patients with SLE and other Rheumatic Diseases [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/study-of-long-term-hcq-safety-on-cardiac-muscle-function-in-patients-with-sle-and-other-rheumatic-diseases/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/study-of-long-term-hcq-safety-on-cardiac-muscle-function-in-patients-with-sle-and-other-rheumatic-diseases/