Session Information
Date: Sunday, October 26, 2025
Title: (0506–0521) Sjögren’s Disease – Basic & Clinical Science Poster I: Etiology, Pathogenesis, Diagnosis
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Salivary Gland Ultrasound (SGUS) can be useful in the evaluation and management of Sjögren’s Disease (SjD) but its use has been limited to trained rheumatologists. We hypothesized that implementation of a standardized scanning protocol and graded according to the Outcome Measures in Rheumatology Clinical Trials (OMERACT) scoring system by an academic radiology department can improve sensitivity for detecting glandular inflammation that may be missed by physical exam.
Methods: This was a retrospective, case-control study of patients with sicca seen in an academic Sjogren’s Center. Patient with SGUS scored as OMERACT grade 3 (≥1 parotid +/- submandibular gland) were compared to OMERACT grade 0 (all glands) with complete serologies (ANA, SSA, RF) available for review. Charts were screened consecutively. For patients with SjD, the EULAR Sjögren’s Disease Activity Index (ESSDAI) and the Routine Assessment of Patient Index Data-3 (RAPID-3) were extracted with demographic, treatment, and laboratory data available either any time prior to the encounter (serologies) or completed up to 3 months after the same encounter. Descriptive statistics, including means and proportions, were calculated and comparisons made by t-test.
Results: Fifty–four patients with grade 3 OMERACT SGUS changes and complete antibody profiles were compared to 54 patients with grade 0 changes. Patients with grade 3 changes had a mean (SD) age of 54.9 years (17.2), were predominantly female (89%), about half met the ACR/EULAR SjD classification criteria (55.6%), and had current use of conventional disease modifying agents (cDMARDs) (48.2%) (Table 1). Patients with grade 3 changes were more likely to have positive serologies (anti-SSA, ANA, RF). In addition, Patients with grade 3 changes had a mean (SD) RAPID-3 score of 9.4 (6.9), indicating moderate disability and symptom burden. For patients diagnosed with SjD with grade 3 changes and completed ESSDAIs (n = 36), the median (IQR) ESSDAI was 3 (0, 6.5) with low activity ( >10%) present in the constitutional, glandular, and articular domains (Table 2). Notably, only 28% of patients with grade 3 SGUS changes had elevated activity levels on the glandular domain of the ESSDAI which is obtained through physical exam (swelling/enlargement of glands).
Conclusion: Patients with OMERACT grade 3 changes on SGUS more often had positive SSA, ANA, and RF compared to those with grade 0 changes. Despite grade 3 changes on SGUS, only 28% of patients had elevated disease activity per ESSDAI glandular domain (physical exam). This may suggest that adoption by general radiology of an SGUS scanning protocol and use of the OMERACT scoring system may improve rheumatologists’ detection of glandular activity, compared to physical exam alone.
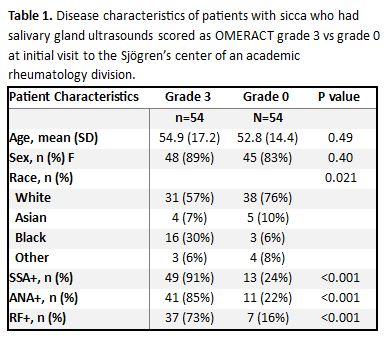 Table 1. Disease characteristics of patients with sicca who had salivary gland ultrasounds scored as OMERACT grade 3 vs grade 0 at initial visit to the Sjögren’s center of an academic rheumatology division.
Table 1. Disease characteristics of patients with sicca who had salivary gland ultrasounds scored as OMERACT grade 3 vs grade 0 at initial visit to the Sjögren’s center of an academic rheumatology division.
.jpg) Table 2. Sjögren’s Disease activity per EULAR Sjögren’s Syndrome Disease Activity Index (ESSDAI) for patients with OMERACT grade 3 changes on salivary gland ultrasound at initial visit. PNS (peripheral nervous system), CNS (central nervous system).
Table 2. Sjögren’s Disease activity per EULAR Sjögren’s Syndrome Disease Activity Index (ESSDAI) for patients with OMERACT grade 3 changes on salivary gland ultrasound at initial visit. PNS (peripheral nervous system), CNS (central nervous system).
.jpg) Figure 1. Qualitative examples of echotexture changes over time from patients who completed 2 SGUSs with grade 3 OMERACT scores.
Figure 1. Qualitative examples of echotexture changes over time from patients who completed 2 SGUSs with grade 3 OMERACT scores.
To cite this abstract in AMA style:
Lee S, Johr C, Sandorfi N, Dhanaliwala A, DiRenzo D. Implementation of Salivary Gland Ultrasound by General Radiology can Improve Detection of Glandular Inflammation in Patients with Sicca [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/implementation-of-salivary-gland-ultrasound-by-general-radiology-can-improve-detection-of-glandular-inflammation-in-patients-with-sicca/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/implementation-of-salivary-gland-ultrasound-by-general-radiology-can-improve-detection-of-glandular-inflammation-in-patients-with-sicca/