Session Information
Date: Sunday, October 26, 2025
Title: (0337–0356) Osteoporosis & Metabolic Bone Disease – Basic & Clinical Science Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Chronic kidney disease (CKD) is linked to increased vascular comorbidity and fracture risk. This study aims to assess bone status in CKD patients versus healthy controls and its relationship with intact fibroblast growth factor 23 (iFGF-23). A secondary aim is to evaluate cardiovascular risk (CVR) in CKD and its associations with bone status and iFGF-23.
Methods: Adults with CKD stages 2–4 (normal phosphate levels) were assessed for bone metabolism, iFGF-23, and bone density using DXA. Bone quality was evaluated via Trabecular Bone Score (TBS) at the lumbar spine and 3D-DXA at the proximal femur. FRAX scores and vertebral fractures were recorded. Carotid ultrasound and Kauppila vascular calcification scores assessed subclinical CVR. A matched control group (age, sex, BMI) was used for bone quality comparison via propensity score matching.
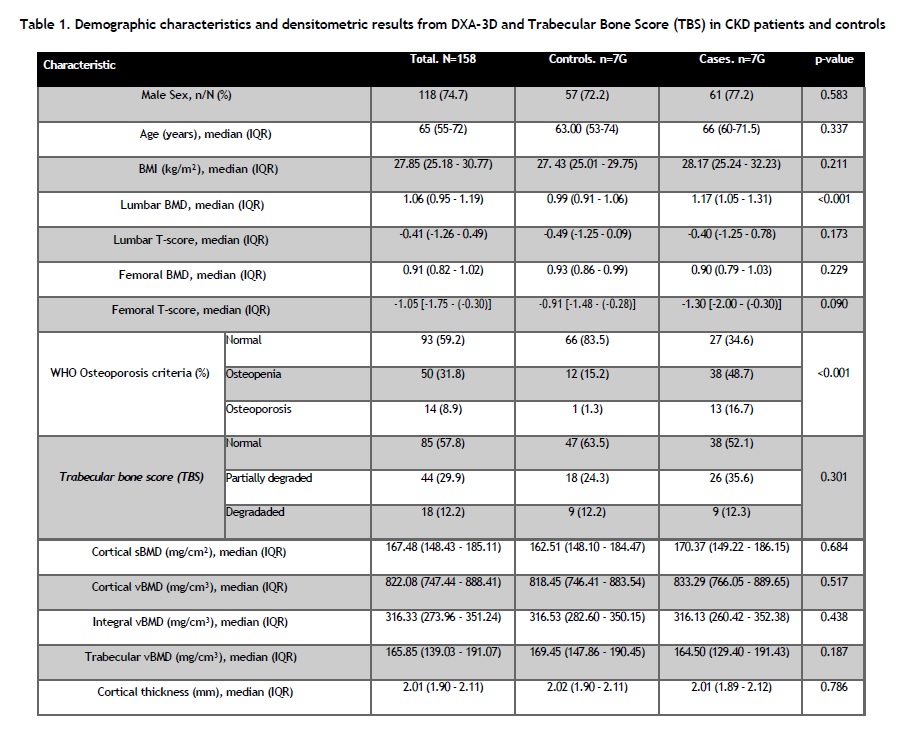
Results: A total of 79 CKD patients were included. Osteoporosis and osteopenia prevalence was higher in CKD patients (16.7% and 48.7%) compared to controls (15.2% and 1.3%,p=0.001). Among CKD patients with vertebral fractures (n=7;10.6%), TBS was lower (1.256 vs. 1.362,p=0.046), and trabecular volumetric BMD (vBMD) by 3D-DXA was reduced (126.5 vs. 166.6 mg/cm³,p=0.019). iFGF-23 inversely correlated with cortical vBMD (ρS: -0.82,p=0.02).No significant differences in BMD, TBS, or 3D-DXA were found between CKD stages G2-G3a and G3b-G4. However, when comparing G2-G3a to controls, osteoporosis and osteopenia were more prevalent (44.7% and 13.2% vs. 15.2% and 1.3%,p=0.001). In G3b-G4 patients versus controls, lower femoral BMD (0.89 vs. 0.93,p< 0.043) and trabecular vBMD by 3D-DXA (161.90 vs. 169.45,p< 0.03) were found, with higher osteoporosis and osteopenia prevalence (52.5% and 20% vs. 15.2% and 1.3%;p=0.001).Table 1 compares demographics and DXA, TBS, and 3D-DXA between CKD patients and controls. Table 2 presents results by CKD stage and controls.In 62 patients undergoing carotid ultrasound (Table 3), 67.7% had low BMD and 50% showed altered TBS. Patients with subclinical CVR and/or cardiovascular disease (CVD) (n=45) were older (p=0.007), with higher carotid intima-media thickness (cIMT, p< 0.001) and Kauppila index (p< 0.001) compared to those without (n=17). DXA, TBS, 3D-DXA did not differ significantly.iFGF-23 inversely correlated with eGFR (r: -0.38, p=0.002). cIMT correlated inversely with 25(OH) vitamin D (r: -0.25, p=0.047), and directly with lumbar BMD (r: 0.485,p< 0.001), cortical vBMD (r: 0.27, p=0.038), cortical surface BMD by 3D-DXA (r: 0.25, p=0.053), and the Kauppila index (r: 0.42,p=0.001).In patients with subclinical CVR and/or CVD and fragility fractures, iFGF-23 was inversely correlated with cortical vBMD (ρS: -0.9,p=0.037).
Conclusion: CKD patients show reduced bone mass compared to healthy individuals, evident even in early stages of the disease. Bone quality alterations assessed by TBS and 3D-DXA may help identify those at risk for vertebral fractures. iFGF-23 appears to contribute to both bone quality deterioration and vascular damage. In the subgroup of patients with subclinical cardiovascular disease and/or major adverse cardiovascular events (MACE) and fragility fractures, impaired bone quality parameters were observed by 3D-DXA.
.jpg)
.jpg)
To cite this abstract in AMA style:
Rodríguez gago J, Tornero C, León L, González-Casaus M, Giraldo L, del Peso G, Garrido D, López T, Coronado M, Bajo M, García S, Serrano M, Ossorio M, Balsa A, Aguado P. Fibroblast Growth Factor-23 and Bone Status in Patients with Chronic Kidney Disease Compared to a Healthy Control Group and Its Relationship with Cardiovascular Risk [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/fibroblast-growth-factor-23-and-bone-status-in-patients-with-chronic-kidney-disease-compared-to-a-healthy-control-group-and-its-relationship-with-cardiovascular-risk/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/fibroblast-growth-factor-23-and-bone-status-in-patients-with-chronic-kidney-disease-compared-to-a-healthy-control-group-and-its-relationship-with-cardiovascular-risk/