Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Lipoprotein subclasses play diverse roles in health and disease. Although lipoproteins have been implicated in knee osteoarthritis (KOA), the relationship between lipoprotein subclasses and KOA remains unexplored.
Methods: We conducted a cohort study of 115,237 participants from the UK Biobank to examine the associations of 85 plasma lipoprotein subclasses, defined by combinations of density (high, low, intermediate, very-low), size (extremely-large, very-large, large, medium, small, very-small), and composition (triglyceride, free cholesterol, cholesteryl ester, phospholipid), with incident KOA in the metabolome-wide analysis (Figure 1A). Data were analyzed using Cox proportional hazards models, correcting for multiple tests (0.05/9). We conducted the analyses using two models. Model 1 adjusted for age, sex, Townsend Deprivation Index score, body mass index (BMI; as a categorical variable), drinking status, smoking status, fasting time, lipid-lowering medication, and history of knee joint injury. Model 2 included the same covariates as Model 1, except that BMI was adjusted as a continuous variable. We subsequently conducted targeted analyses to examine the association between the key lipoprotein subclasses, which consistently showed significant associations with KOA across both models, and knee replacement, as the outcome may reflect severe OA (Figure 1B).
Results: During a median follow-up period of 12.8 years, 6,782 incident cases of KOA were identified. A total of 38 lipoprotein subclasses were statistically significantly associated with incident KOA (Figure 2). Specifically, higher concentrations of very-large and large high-density lipoproteins (HDL), excluding triglyceride, were associated with a lower risk of incident KOA (hazard ratios [HRs] range 0.87-0.94). Conversely, higher concentrations of small HDL, irrespective of composition, were associated with a higher risk of incident KOA (HRs range 1.04-1.09). Extremely-large very-low-density lipoprotein (VLDL) across all compositions, very-large VLDL excluding cholesteryl ester, and large VLDL excluding cholesteryl ester showed positive associations with incident KOA (HRs range 1.05-1.10). Additionally, medium, small, and very-small VLDL, and intermediate-density lipoprotein, as well as large, medium and small low-density lipoprotein, combined with triglyceride, were consistently positively associated with incident KOA (HRs range 1.04-1.06). After adjusting for BMI as a continuous variable, differential effects among HDL subclasses remained evident, except for the association between large HDL and KOA. Conversely, the associations between other lipoprotein subclasses and KOA become non-statistically significant. Similar findings were observed for the associations between HDL subclasses and the risk of knee replacement in the targeted analysis (Figure 3).
Conclusion: We provided novel evidence of diverse associations between lipoprotein subclasses and incident KOA, indicating the distinct effects of HDL subclasses.
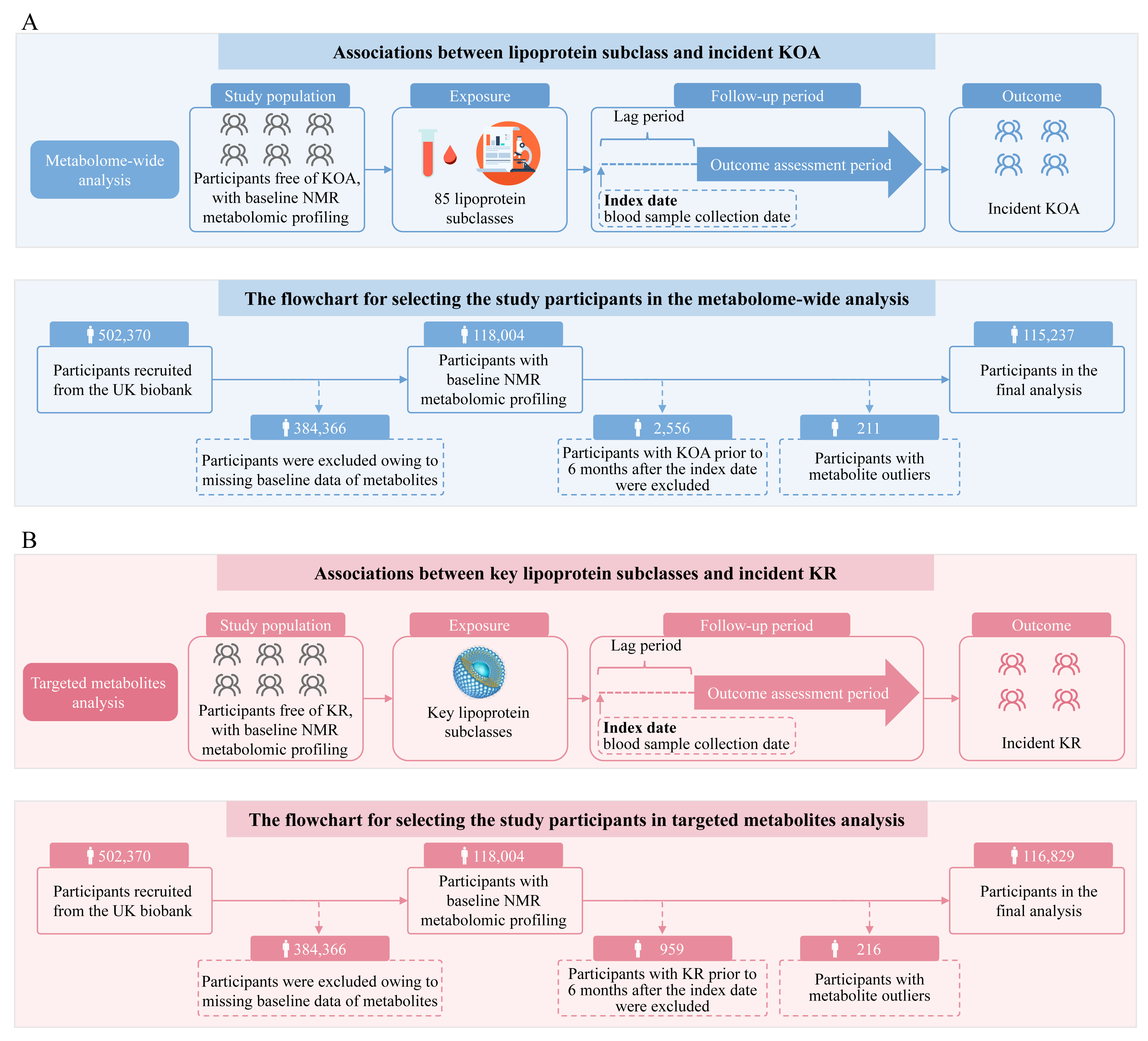 Figure 1: The schematic illustration of this study. (A) Part 1: Metabolome-wide analysis for the associations of 85 lipoprotein subclass and the risk of incident KOA; Part 2: Flowchart for the selection of the study population for metabolome-wide analysis. (B) Part 1: Targeted analysis for the associations of key lipoprotein subclass and the risk of incident KR; Part 2: Flowchart for the selection of the study population for targeted analysis. The date of blood sample collection was designated as the index date for each participant. Key lipoprotein subclasses were defined as those that showed consistent significant associations with KOA across both models in the metabolome-wide analysis. KOA, knee osteoarthritis; KR, knee replacement; NMR, nuclear magnetic resonance.
Figure 1: The schematic illustration of this study. (A) Part 1: Metabolome-wide analysis for the associations of 85 lipoprotein subclass and the risk of incident KOA; Part 2: Flowchart for the selection of the study population for metabolome-wide analysis. (B) Part 1: Targeted analysis for the associations of key lipoprotein subclass and the risk of incident KR; Part 2: Flowchart for the selection of the study population for targeted analysis. The date of blood sample collection was designated as the index date for each participant. Key lipoprotein subclasses were defined as those that showed consistent significant associations with KOA across both models in the metabolome-wide analysis. KOA, knee osteoarthritis; KR, knee replacement; NMR, nuclear magnetic resonance.
.jpg) Figure 2: Associations of individual lipoprotein metabolites with risk of incident KOA. HRs (per SD) were adjusted for age, sex, Townsend Deprivation Index score, body mass index, drinking status, smoking status, fasting time, lipid-lowering medication, and history of knee joint injury. The red bars indicate HR>1, while the blue bars represent HR < 1. The significant lipoprotein metabolites are highlighted in bold. *P < 5.6×10-3 (0.05/9). KOA, knee osteoarthritis; HR, hazard ratios; SD, standard deviation; -CE, cholesteryl ester; -FC, free cholesterol; HDL, high-density lipoprotein; IDL, intermediate-density lipoprotein; L-, large; LDL, low-density lipoprotein; M-, medium; -P, particle concentration; PL, phospholipids; S-, small; TG, triglycerides; VLDL, very-low-density lipoprotein; XL-, very-large; XS-, very-small; XXL-, extremely-large.
Figure 2: Associations of individual lipoprotein metabolites with risk of incident KOA. HRs (per SD) were adjusted for age, sex, Townsend Deprivation Index score, body mass index, drinking status, smoking status, fasting time, lipid-lowering medication, and history of knee joint injury. The red bars indicate HR>1, while the blue bars represent HR < 1. The significant lipoprotein metabolites are highlighted in bold. *P < 5.6×10-3 (0.05/9). KOA, knee osteoarthritis; HR, hazard ratios; SD, standard deviation; -CE, cholesteryl ester; -FC, free cholesterol; HDL, high-density lipoprotein; IDL, intermediate-density lipoprotein; L-, large; LDL, low-density lipoprotein; M-, medium; -P, particle concentration; PL, phospholipids; S-, small; TG, triglycerides; VLDL, very-low-density lipoprotein; XL-, very-large; XS-, very-small; XXL-, extremely-large.
.jpg) Figure 3: Associations of the key lipoprotein subclass with the risk of incident knee replacement. HRs (per SD) were adjusted for age, sex, Townsend Deprivation Index score, body mass index, drinking status, smoking status, fasting time, lipid-lowering medication, and history of knee joint injury. HR, hazard ratio; SD, standard deviation; CI, confidence interval; HDL, high-density lipoprotein.
Figure 3: Associations of the key lipoprotein subclass with the risk of incident knee replacement. HRs (per SD) were adjusted for age, sex, Townsend Deprivation Index score, body mass index, drinking status, smoking status, fasting time, lipid-lowering medication, and history of knee joint injury. HR, hazard ratio; SD, standard deviation; CI, confidence interval; HDL, high-density lipoprotein.
To cite this abstract in AMA style:
Li C, wu J, Zhang Y, He H, Hu Y, Wei J, Lei G, Zeng C. Plasma Lipoprotein Subclasses and Risk of Incident Knee Osteoarthritis: A Population-Based Cohort Study [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/plasma-lipoprotein-subclasses-and-risk-of-incident-knee-osteoarthritis-a-population-based-cohort-study/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/plasma-lipoprotein-subclasses-and-risk-of-incident-knee-osteoarthritis-a-population-based-cohort-study/